


A 51-year-old man with no significant medical history presented to the emergency department with fever and dyspnea lasting for 10 days. On presentation, his body temperature was 36.6°C (97.9°F), respiratory rate 15 breaths per minute, and oxygen saturation 90% on 1 L per minute of oxygen.
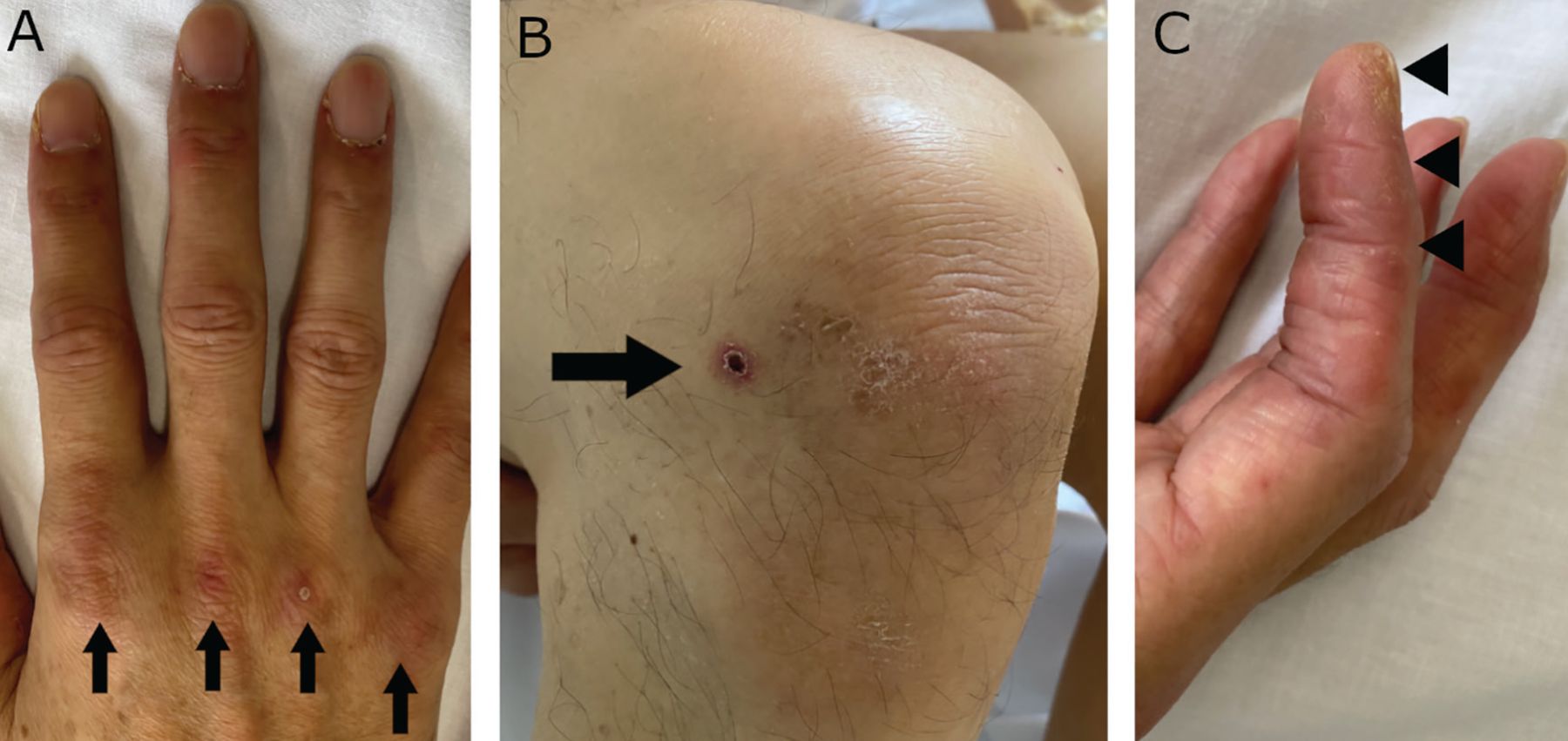
On physical examination, fine crackles were heard bilaterally at the base of the lungs. No evidence of muscle weakness was observed. Skin examination (Figure 1) revealed Gottron papules at the knees, elbows, and meta-carpophalangeal joints of the hands, a skin ulcer at the knee, hyperkeratosis of the lateral aspect of the index finger of both hands, periungual erythema, and palmar papules.
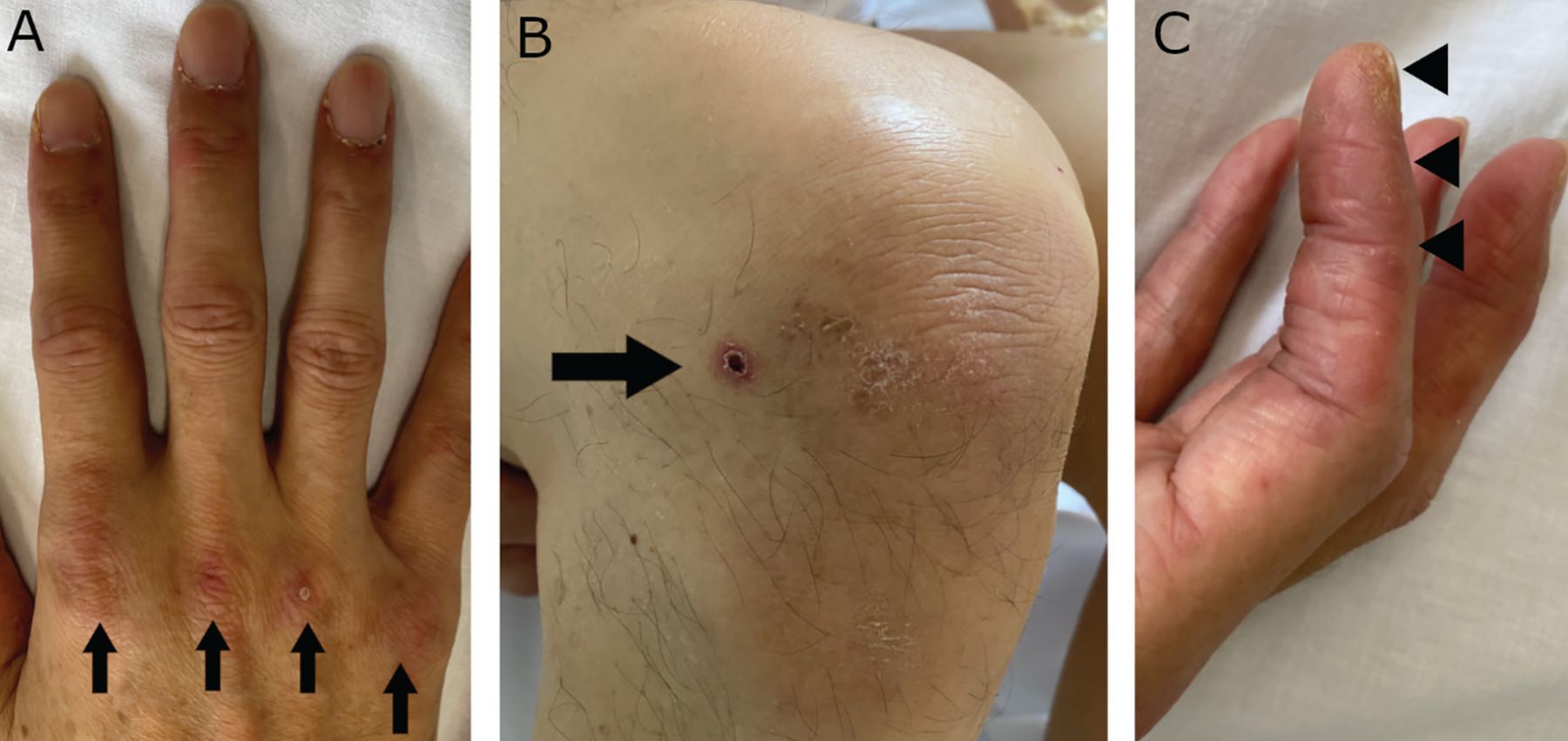
Examination of the patient revealed (A) Gottron sign (arrows), (B) ulceration on the right knee (arrow), and (C) linear hyperkeratotic lesions on the radial aspect of the index finger (“mechanic’s hands”).
Results of initial laboratory testing were as follows:
Leukocyte count 10.7 × 109/L (reference range 3.3–8.6 × 109/L)
Creatine kinase 257 IU/L (reference range 59–248 IU/L)
Ferritin 841.8 ng/mL (reference range 39–340 ng/mL)
C-reactive protein 5.5 mg/dL (reference range 0–0.14 mg/dL).
Chest computed tomography (CT) (Figure 2) revealed bilateral peripheral subpleural ground-glass opacities in the upper and lower lobes.
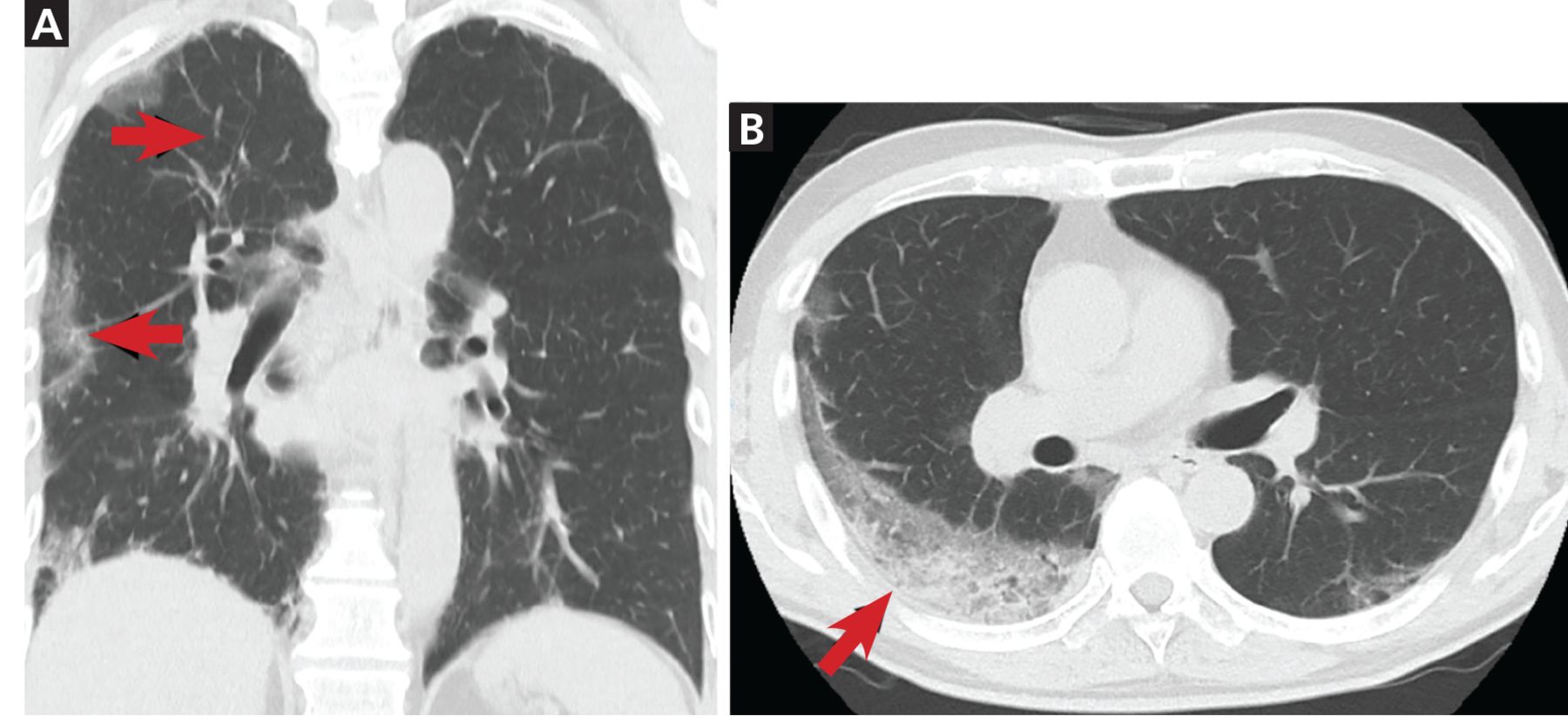
Computed tomography of the chest revealed peripheral subpleural ground-glass opacities in the right upper lobe (A, arrows) and right lower lobe (B, arrow).
In the emergency department, interstitial pneumonia including COVID-19 pneumonia was suspected, but SARS-CoV-2 real-time polymerase chain reaction testing of nasopharyngeal swabs and a sputum specimen was negative. Consultation with the rheumatology department and review of the clinical findings led to a diagnosis of rapidly progressive interstitial lung disease (ILD) associated with dermatomyositis.
The hyperkeratosis of the lateral digit suggested “mechanic’s hands.” The characteristic skin findings, lack of muscle symptoms, and progressive pneumonia led to the clinical diagnosis of amyopathic dermatomyositis. In addition, we ordered testing for anti-melanoma differentiation-associated gene 5 (anti-MDA5) antibody on admission, but results were not immediately available
Treatment with methylprednisolone pulse therapy, intravenous cyclophosphamide pulse therapy, and tacrolimus was promptly initiated, and his respiratory status gradually improved. Later, the test for anti-MDA5 was confirmed positive, thus further refining the diagnosis to anti-MDA5-positive dermatomyositis with ILD.
ANTI-MDA5-POSITIVE DERMATOMYOSITIS AND THE DIFFERENTIAL DIAGNOSIS OF ILD
Anti-MDA5-positive dermatomyositis is a subtype of myositis with characteristic skin rashes and ulcers, amyopathic or hypomyopathic symptoms, and rapidly progressive ILD.1,2 It is associated with a poor prognosis, with 6-month survival rates of 33% to 50%.2–4
Early diagnosis and early intervention are necessary to improve the prognosis.4,5 Although standard treatment has not been established, combination therapy of high-dose glucocorticoids (1 mg/kg), a calcineurin inhibitor (cyclosporine A or tacrolimus), and intravenous cyclophosphamide should be considered as first-line therapy.4,5 In refractory cases, concomitant use of rituximab as salvage therapy has been reported to be effective.5 For patients who do not respond to combination therapy, nonpharmacologic therapies such as plasma exchange and intravenous immunoglobulin are considered options, but their efficacy has not yet been proven.5
CT in our patient showed bilateral peripheral subpleural ground-glass opacities in the lower lobes, with findings similar to those of viral pneumonia or ILD.1,2
Anti-MDA5-positive dermatomyositis with ILD triggered by a viral infection has been reported, although viral infection has not been directly proven as the mechanism underlying this condition.2
DIFFERENTIATING ILD FROM COVID-19
In the context of the COVID-19 pandemic, a detailed history and physical examination are particularly important for the differential diagnosis of ILD. Muscle weakness and elevated muscle enzyme are often absent or scant in anti-MDA5-positive dermatomyositis, making the diagnosis of dermatomyositis difficult.
The key to diagnosis is the characteristic skin findings such as Gottron papules, skin ulcers, palmar papules, and lateral digit hyperkeratosis. It is important not to overlook the minor skin findings that are present with pneumonia.2
COVID-19 also shows a variety of skin findings such as perniolike lesions and urticarial and morbilliform rashes, but cutaneous ulceration is rare.6 Cutaneous ulceration overlying Gottron papules is one of the most characteristic signs and is present in 83% of patients with anti-MDA5-positive dermatomyositis.2
Anti-MDA5-positive dermatomyositis with ILD mimics COVID-19 and is a reminder of the importance of careful physical examination for diagnosis.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}