


A 75-year-old man presented to the hospital with altered mental status and pancytopenia. He had a history of schizophrenia and gastrointestinal bleeding due to peptic ulcer disease, for which he had undergone subtotal gastrectomy.
Results of a complete blood cell count at presentation showed the following:
Hemoglobin 5.5 g/dL (reference range 14.5–18.1)
Hematocrit 17.5% (42.0–54.0)
Mean corpuscular volume 108.7 fL (80–100)
White blood cell count 3.5 × 109/L (4.41–10.05)
Platelet count 54 × 109/L (150–400)
Lactate dehydrogenase 3,320 U/L (90–285)
Haptoglobin < 10 mg/dL (33–171)
Total bilirubin 2.6 mg/dL (< 1.2)
Indirect bilirubin 1.8 mg/dL (< 1.2).
Results of an iron panel study were consistent with anemia of chronic inflammation with serum iron 177 μg/dL (40–150), total iron binding capacity 179 μg/dL (280–500), iron saturation 98.89%, and ferritin 408 ng/ mL (40–400). The reticulocyte percentage was 1% with a reticulocyte index of 0.17%, indicating a hypoproliferative type of anemia.
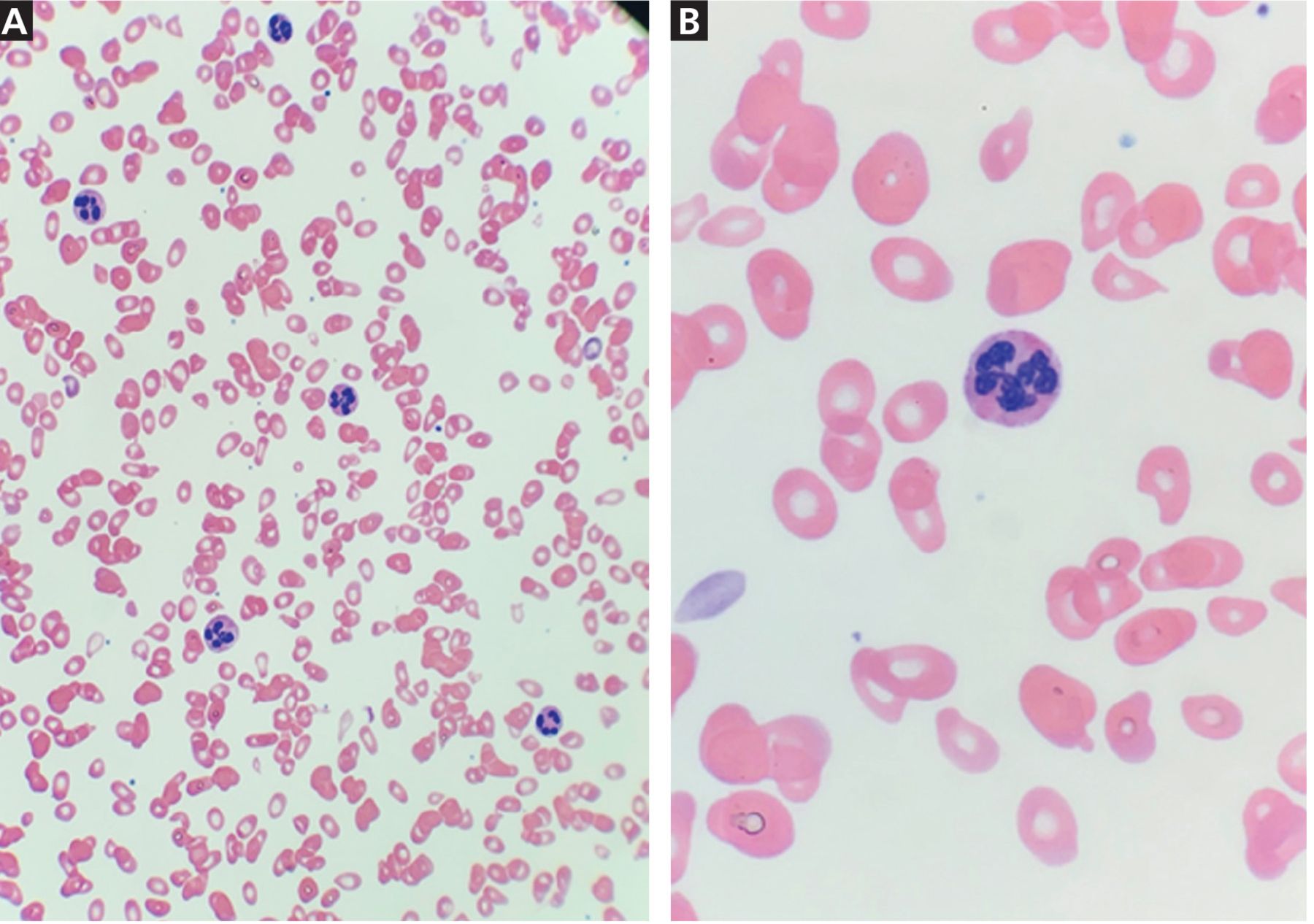
In addition, the vitamin B12 level was low at 93 pg/mL (220–600), serum folate was normal at 8.2 ng/mL (> 3), homocysteine was elevated at 138 μmol/L (0.0–19.2), and methylmalonic acid was elevated at 25,024 nmol/L (0.0–378). A peripheral blood smear (Figure 1) showed the presence of macrocytosis, thrombocytopenia, and hypersegmented neutrophils (ie, with multiple lobes in nuclei). These findings, consistent with megaloblastic anemia, confirmed the diagnosis of megaloblastic anemia due to vitamin B12 deficiency.
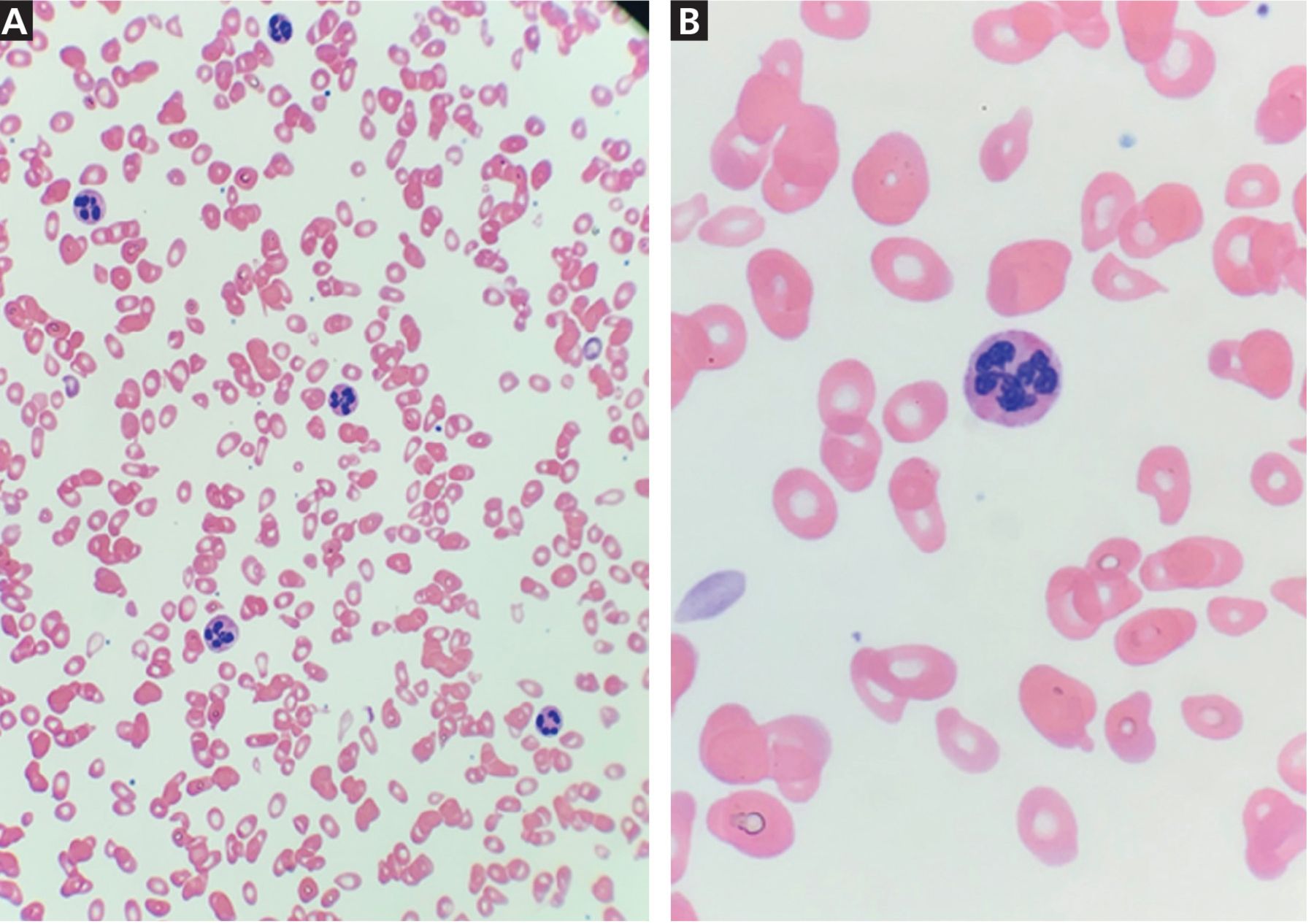
Peripheral blood smears show hypersegmented neutrophils consistent with megaloblastic anemia. Panel A (hematoxylin and eosin, magnification × 40) shows neutrophils with hypersegmented multilobed nuclei (more than 5 lobes, dark blue stain) in a background of anisocytosis with macrocytes, ovalocytes, and thrombocytopenia. Panel B (hematoxylin and eosin, magnification × 100) shows a neutrophil (stained dark blue) with multilobed nuclei.
MEGALOBLASTIC ANEMIA: DIAGNOSTIC CLUES
Macrocytic and megaloblastic anemia from vitamin B12 deficiency leads to defective DNA synthesis in hematopoietic precursors manifesting as pancytopenia and hemolysis owing to ineffective hematopoiesis. Megaloblastic anemia is commonly related to vitamin B12 or folate deficiency.1–4 Important differential diagnoses to consider include medication side effects (eg, methotrexate, chemotherapy, or antibiotics such as trimethoprim), and malabsorption due to an anatomic or autoimmune cause (pernicious anemia), as well as a primary bone marrow pathology such as myelodysplastic syndrome.
In this patient, megaloblastic anemia was diagnosed based on clinical and laboratory findings of severe vitamin B12 deficiency, for which subtotal gastrectomy is a known predisposing factor.
CASE CONCLUSION
The patient was immediately started on vitamin B12 1,000 μg weekly by intramuscular injection. Several days after the start of treatment, repeat testing showed improving bone marrow recovery, with an increase in reticulocyte count and normalization of lactate dehydrogenase. At 2 weeks, the patient experienced significant improvement in complete blood cell count and mental status.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}