


Article Figures & Data
Figures
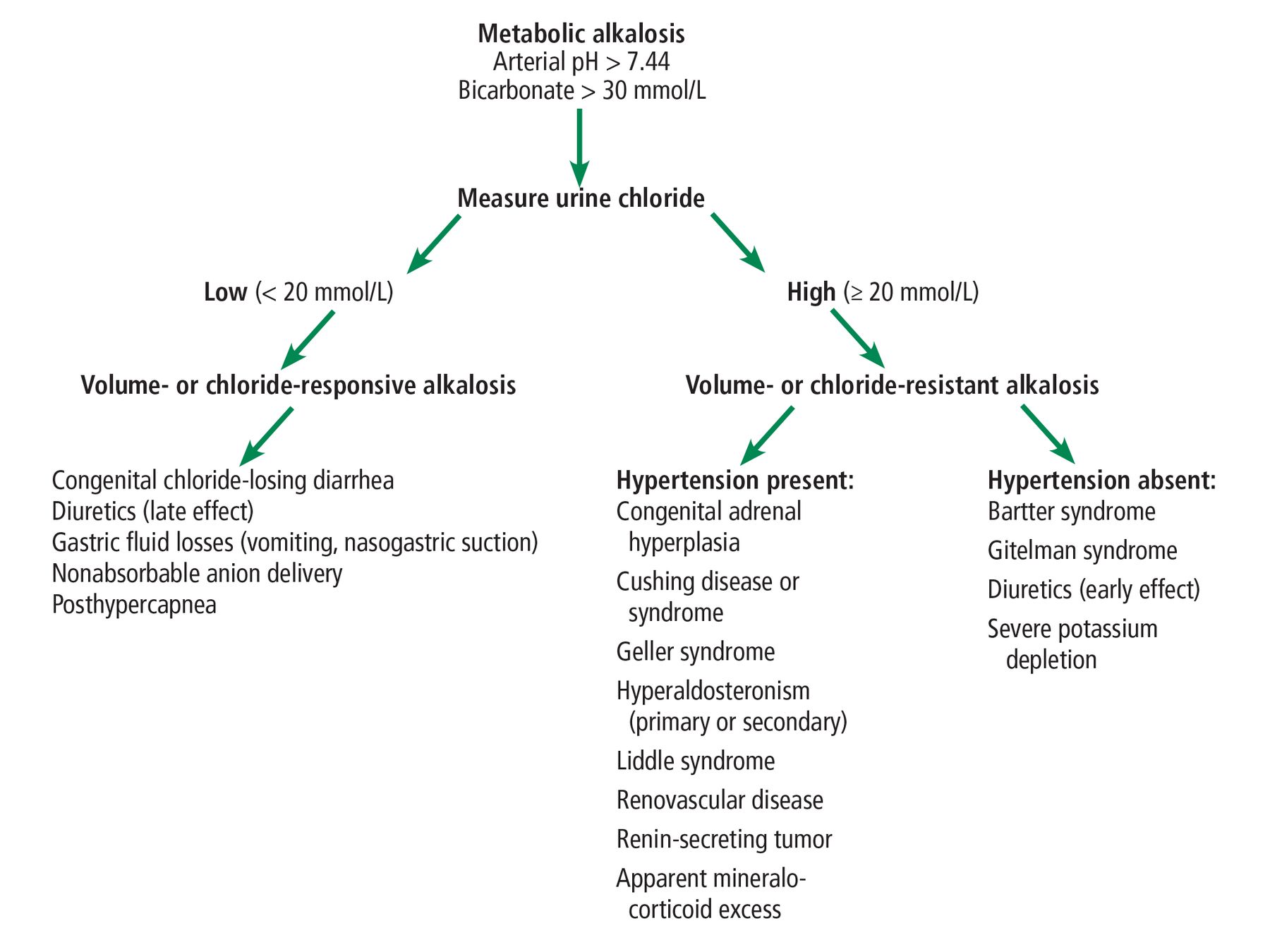
- Figure 1
Metabolic alkalosis should first be evaluated by obtaining a random urine chloride. This step helps classify it as volume-responsive (urine chloride < 20 mmol/L) or volume-resistant (urine chloride ≥ 20 mmol/L). The latter is further divided based on the presence or absence of hypertension.
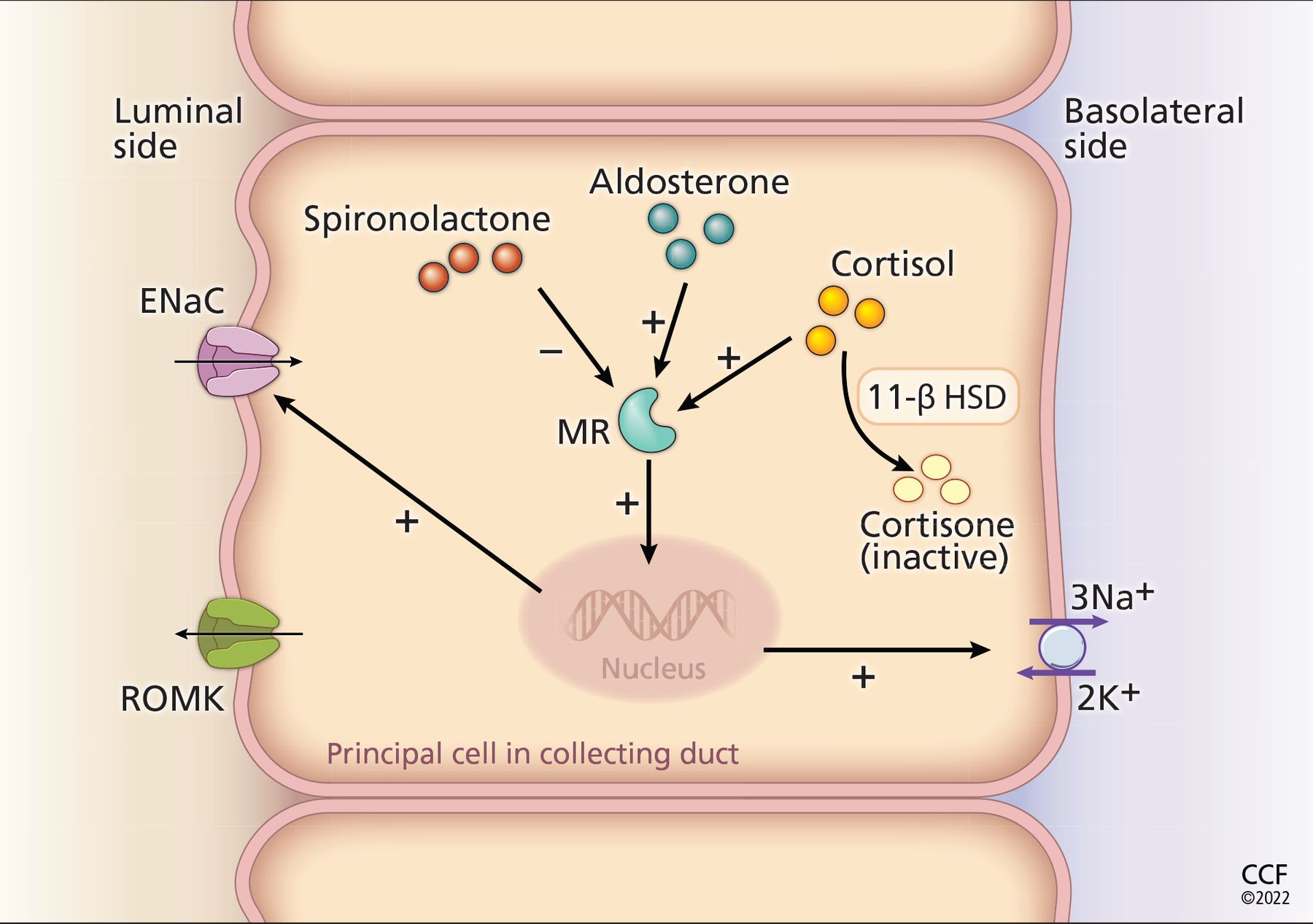
- Figure 2
Processes of mineralocorticoid excess and effect of spironolactone. In the principal cells in the collecting ducts of the kidney, activation of the mineralocorticoid receptor (MR) increases the transcription, translation, and insertion of more epithelial sodium channels (ENaC) in the luminal side. Cortisol and aldosterone have the same affinity for the mineralocorticoid receptor, but aldosterone is present in higher concentrations. Activation of the mineralocorticoid receptor stimulates a cascade of intracellular reactions that results in increased expression of the epithelial sodium channel. Spironolactone blocks the mineralocorticoid receptor. The enzyme 11-β hydroxysteroid dehydrogenase (HSD) type 2 converts cortisol to its inactive metabolite, cortisone. This enzyme can be absent in apparent mineralocorticoid excess, or it can be inhibited by licorice or posaconazole. Notably, the increased number of epithelial sodium channels leads to sodium (Na+) reabsorption from the tubular lumen. To maintain electroneutrality, another positive ion (K+) is secreted into the tubular lumen through the renal outer medullary potassium channel (ROMK).

Tables
Test Resultsa Reference range Sodium 140 mmol/L 132-148 mmol/L Potassium 2.1 mmol/L 3.5-5.0 mmol/L Chloride 93 mmol/L 98-111 mmol/L Bicarbonate > 45 mmol/L 23-32 mmol/L Blood urea nitrogen 30 mg/dL 10-25 mg/dL Creatinine 1.11 mg/dL 0.7-1.4 mg/dL Calcium 8.0 mg/dL 8.4-10.5 mg/dL Albumin 2.7 g/dL 3.5-5.0 g/dL Hemoglobin A1c 6.8% < 5.7% Hemoglobin 14.5 g/dL 12-16 g/dL White blood cell count 14.3 x 109/L 3.7-11.0 x 109/L Platelet count 79 x 109/L 140-400 x 109/L Alanine aminotransferase 79 U/L 0-45 U/L Aspartate aminotransferase 81 U/L 7-40 U/L Alkaline phosphatase 129 U/L 40-150 U/L Bilirubin, total 1.4 mg/dL 0-1.5 mg/dL Arterial blood gasses PH 7.55 7.35-7.45 Pco2 54 mm Hg 35-45 mm Hg PO2 34 mm Hg 75-100 mm Hg Bicarbonate 47 mmol/L 18-23 mmol/L ↵a Abnormal results are shown in bold.
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- METABOLIC DISTURBANCES REVIEWED
- FURTHER EVALUATION OF METABOLIC ALKALOSIS
- CASE CONTINUED: RESULTS OF FURTHER TESTING
- CAUSES OF VOLUME-RESISTANT METABOLIC ALKALOSIS WITH LOW RENIN AND ALDOSTERONE
- CASE CONTINUED: A CANCER DIAGNOSIS
- ANTIHYPERTENSIVE THERAPY IN HYPERMINERALOCORTICOID STATES
- CASE CONCLUSION
- TEACHING POINTS
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.