


A 30-year-old woman came to the emergency department with episodes of weakness and presyncope, as well as constipation, nausea, vomiting, and salt-craving. The symptoms had begun 9 months earlier, after a miscarriage at 10 weeks of pregnancy, and had increased in frequency. She had also noticed dark colorations on her lower lip and inner cheek, which her primary physician had told her might be due to ink from a pen.
She also said that after searching the Internet for conditions that included her symptoms, she was convinced that she had Addison disease.
INITIAL MANAGEMENT AND WORKUP
Intravenous fluids were initiated for her symptoms of weakness and presyncope.
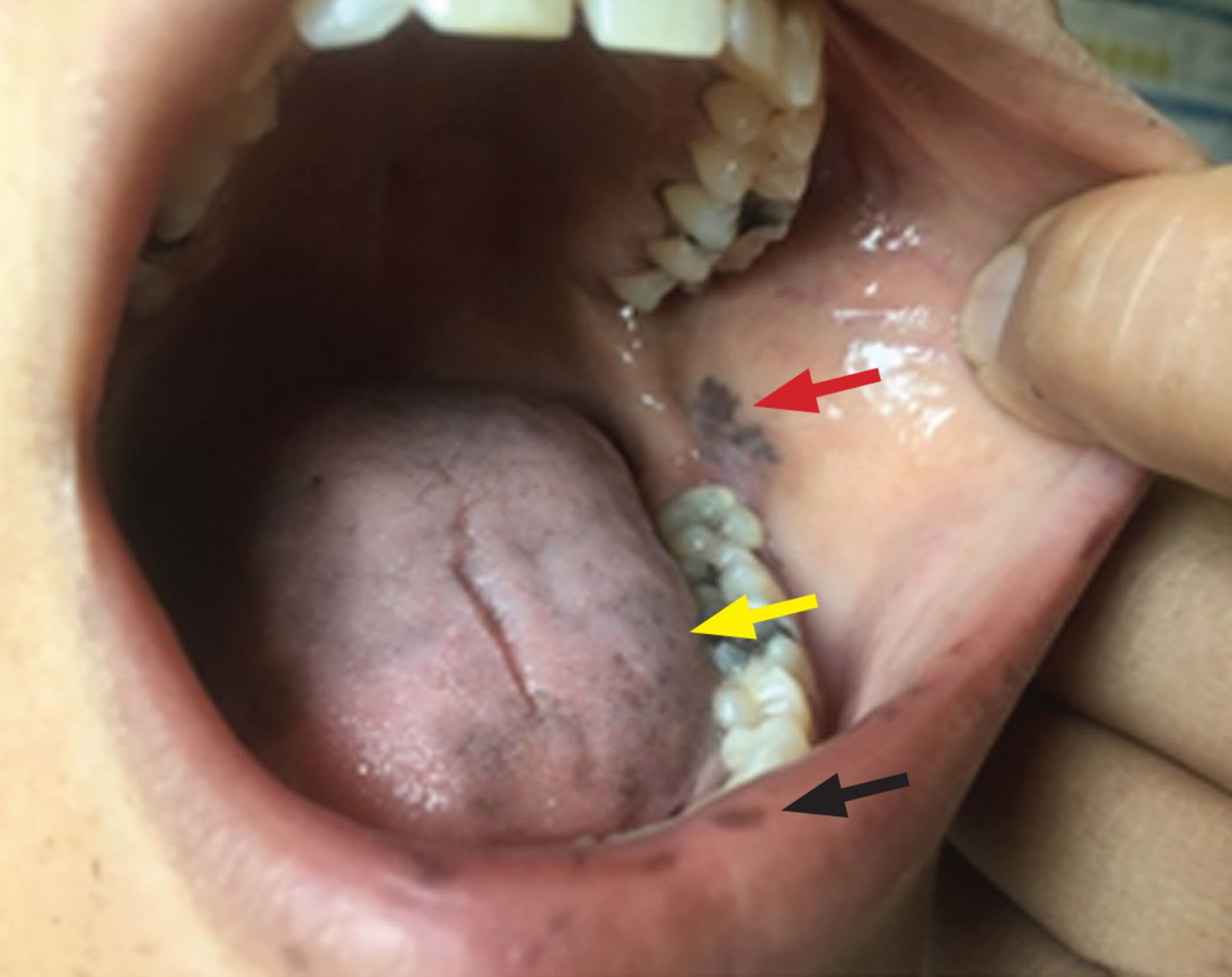
Physical examination demonstrated generalized cutaneous hyperpigmentation involving the lips, tongue, and buccal mucosa (Figure 1), as well as the gums and palmar creases.
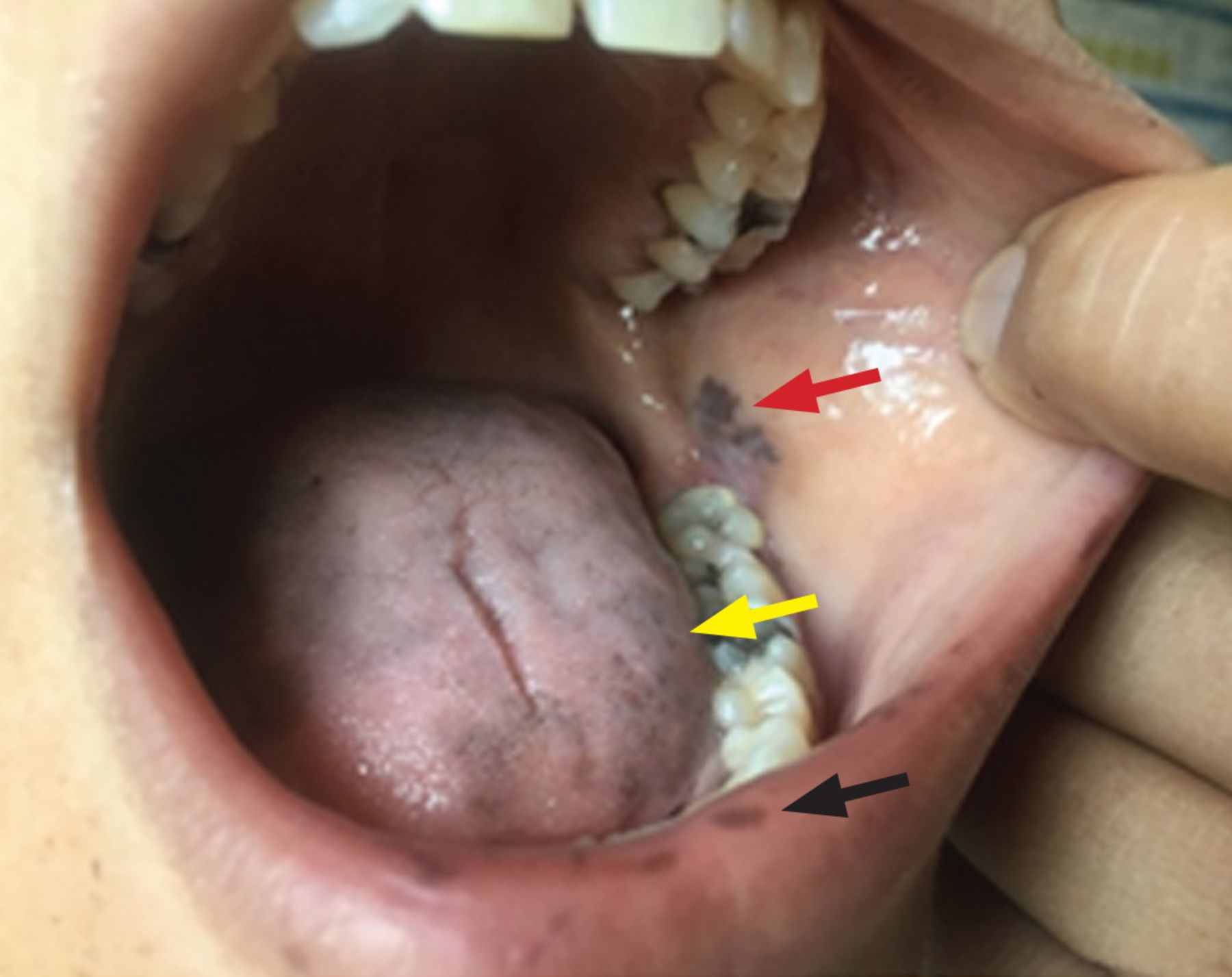
Hyperpigmented lesions involved the lower lip (black arrow), tongue (yellow arrow), and buccal mucosa (red arrow).
Laboratory testing revealed a cortisol level of 0.8 μg/dL (reference range 3.10–22.40) and adrenocorticotropic hormone (ACTH) greater than 1,250 pg/mL (0.00–45.99). Intravenous saline and hydrocortisone succinate were initiated. The thyroid-stimulating hormone level was slightly elevated and, of note, her electrolytes and blood urea nitrogen-to-creatinine ratio were normal at the time of presentation to the emergency department. She was transitioned to hydrocortisone and fludrocortisone the next day.
ADDISON DISEASE: KEY FEATURES
In the United States and Western Europe, Addison disease has a prevalence of 1 in 20,000 persons, higher in women than in men.1 The diagnosis is challenging due to the nonspecific constitutional symptoms, which are frequently mistaken for psychiatric disorders, extra-adrenal gastrointestinal endocrine disorders, or other endocrine disorders such as hypothyroidism.2 The symptoms are subtle and often insidious and can include hyperpigmentation, anorexia, nausea, and fatigue. Elevated ACTH levels and lack of a rise in cortisol levels after an ACTH stimulation test confirm the diagnosis. In our patient, the almost undetectible cortisol level combined with extremely high ACTH level confirmed primary adrenal insufficiency and obviated the need for a formal ACTH-stimulation test.
The mainstay of treatment is lifelong oral hormone replacement therapy with glucocorticoids and mineralocorticoids at doses sufficient to keep electrolytes and plasma renin activity levels in the upper limits of normal.3,4
Addisonian crisis
Undiagnosed Addison disease may lead to addisonian crisis, a life-threatening acute cortisol deficiency presenting as a rapid clinical decompensation to obtundation, encephalopathy, and shock, requiring emergency administration of intravenous fluids and parenteral glucocorticoids to prevent circulatory collapse.5,6 A high index of suspicion and early diagnosis are paramount.
Adrenal insufficiency causes hyponatremia through insufficient excretion of free water and sodium wasting.7 In a retrospective multicenter study of patients with autoimmune Addison disease,8 of 247 patients for whom sodium concentrations were available, hyponatremia was present in 84% (207) and was the most consistent biochemical finding of Addison disease. Many patients may have concurrent autoimmune thyroiditis with high levels of thyroid-stimulating hormone.8 Introducing thyroxine replacement before steroid replacement may cause addisonian crisis.8,9
CASE CONCLUSION AND TAKE-HOME MESSAGE
Our patient’s case illustrates how misattributing hyperpigmented lesions on the lip, tongue, and buccal mucosa as due to pen ink in a patient with symptoms of weakness, presyncope, salt-craving, nausea, and vomiting delayed the diagnosis of this potentially life-threatening disease. In this case, the patient’s own Internet search raised suspicion of adrenal insufficiency.
At 6 months after her presentation to the emergency department, she had gained about 10 pounds, with no recurrence of the periods of weakness. Her buccal hyperpigmentation also appeared to be lightening.
Thus, in a patient presenting with new onset of oral hyperpigmentation, clinicians should consider the pigmented lesions in the context of clinical symptoms with a high degree of suspicion for Addison disease.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.