


ABSTRACT
Psychogenic nonepileptic seizure (PNES) is often misdiagnosed as epilepsy, leading to unnecessary treatments and procedures, as well as failure to engage patients in needed mental health care. To establish an accurate diagnosis, video electroencephalography (EEG) in the context of and simultaneous with a comprehensive neurologic and psychosocial evaluation is recommended for any patient with seizures that are not responding to treatment. Delivering the diagnosis with empathy and respect is a crucial component of care that helps patients establish trust with caregivers and follow treatment recommendations. Effective treatment is available, highlighting the importance of early diagnosis to avoid unnecessary and potentially harmful treatment. But there are many barriers to care, including provider misperceptions, lack of acceptance of the diagnosis, poor patient engagement with treatment, and lack of access to care.
PNES resembles epileptic seizure in signs and symptoms but is due to psychological distress, a form of conversion disorder.
PNES is frequently misunderstood as being consciously feigned, and patients often feel accused of “faking” their seizures.
Inpatient video EEG in an epilepsy monitoring unit is the gold standard for diagnosis.
Psychotherapy should be tailored to the predisposing, perpetuating, and precipitating factors that contributed to the development of PNES.
A 19-year-old right-handed man who had meningitis at age 12 presented with seizures that had begun 12 months earlier. He described the seizures as bilateral arm-stiffening and stuttering speech, followed by rocking movements of the head and trunk that waxed and waned over 30 to 40 minutes. He said he never lost consciousness. He identified lack of sleep and stress as triggers.
The patient was brought to a local emergency department in the midst of a prolonged seizure and was treated with intravenous lorazepam. He was evaluated by a local neurologist, who prescribed levetiracetam for the seizures. Results of routine outpatient electroencephalography (EEG) and brain magnetic resonance imaging were normal. He continued to have seizures, despite escalation of levetiracetam doses.
See related article, page 260
He was admitted to the epilepsy monitoring unit for continuous video EEG monitoring. Several typical episodes were recorded and confirmed by family members and the patient. The episodes were characterized by gradual onset of irregular jerking of his head and arms, followed by arm and truncal stiffening and initial eyes-closed unresponsiveness. He then gradually started following commands but continued to have irregular bilateral jerking movements for 10 more minutes. No epileptiform EEG changes were seen before, during, or after the episodes. Likewise, interictal EEG over 72 hours was normal. He was diagnosed with psychogenic nonepileptic seizure (PNES).
PREVIOUSLY KNOWN AS PSEUDOSEIZURE
Previously known as pseudoseizure, PNES resembles epileptic seizures in symptoms and signs but is not caused by abnormal epileptiform electrical activity in the brain. Instead, this disorder is a manifestation of underlying psychological distress and unresolved emotions. Many people diagnosed with PNES meet the criteria for conversion disorder (also known as functional neurological symptom disorder) or other somatoform disorder, and others meet the criteria for dissociative disorder.
Multiple terms have been used to describe PNES, including dissociative seizure, functional seizure, stress seizure, and nonepileptic attack, reflecting the difficulty of finding a term that respectfully indicates both the psychological nature of the condition and its superficial similarity to epilepsy. The long-entrenched term pseudoseizure has been misinterpreted by patients and physicians as meaning the patient is “faking” or feigning the seizures. Unfortunately, this view has negatively influenced how some healthcare providers treat patients with PNES.
Importantly, there are other causes of nonepileptic events besides PNES—eg, syncope, migraine (which can be accompanied by transient focal neurologic symptoms and signs), paroxysmal dystonias, and other movement disorders. Rarely, a nonepileptic event is due to intentional deception as in factitious disorder or malingering. In some people with developmental or intellectual disabilities, nonepileptic events are behavioral or attention-seeking. PNES is distinctly different in that it is not conscious or intentional.
PATHOPHYSIOLOGY
The pathophysiology of PNES is unclear, but the literature suggests PNES is a network disorder affecting sensorimotor processing, emotional regulation, and neural responses to stress.1 Functional neuroimaging studies provide some evidence that people with PNES have abnormalities in limbic brain structures including the amygdala, hippocampus, parahippocampal gyrus, insula, cingulate cortex, and prefrontal cortex.2
EPIDEMIOLOGY
PNES can develop at any age but is most common between ages 15 and 35.
The disorder is more common in women, and particularly in women who have been victims of abuse.3 Childhood abuse (sexual, emotional, or physical) is strongly correlated with subsequent development of PNES.4 Psychiatric disorders such as depression, anxiety, and posttraumatic stress disorder (PTSD) are also commonly seen in patients with PNES, as discussed further below.
Early studies estimated the prevalence of PNES at 2 to 33 per 100,000.5 A 2021 systematic review calculated the incidence of PNES in the United States at 3.1 per 100,000 per year, and the prevalence at 108.5 per 100,000.6 In a 2021 population-based study in Norway, the mean annual incidence of PNES was also found to be 3.1 per 100,000 per year; the prevalence was 23.8 per 100,000, with the highest prevalence among 15- to 19-year-olds at 59.5 per 100,000.7 In comparison, epilepsy has an incidence of 62 per 100,000 per year8 and a prevalence of 1.2%, or 1,200 per 100,000.9
From 25% to 35% of patients referred to epilepsy monitoring units for video EEG are diagnosed with PNES.10,11 The disorder is often misdiagnosed as epilepsy, placing patients at risk of iatrogenic complications related to unnecessary antiseizure medications and inappropriate medical interventions such as intensive care unit admission, benzodiazepine administration, and oral intubation. In a study of 384 patients diagnosed with status epilepticus and treated unsuccessfully with benzodiazepines, 10% were ultimately determined to have PNES.12
PNES is associated with poor quality of life13 and high rates of unemployment and disability.14 Mortality rates are also higher in people with PNES than in the general population, with one study finding that 20% of deaths in those with PNES under age 50 were due to suicide.15
DIAGNOSED BY HISTORY AND VIDEO EEG
A comprehensive history and video EEG during a typical seizure are the gold standard for diagnosing PNES. There should be no epileptiform abnormalities on the EEG before, during, or after a typical event.
Absence of EEG changes alone, however, is not always diagnostic. EEG must be interpreted in the context of clinical signs and symptoms. Features of seizure semiology or symptomatology that are highly predictive of PNES include long duration of convulsive-type seizures (> 10 minutes), convulsive-type seizures with retained awareness, rapid side-to-side head movements, out-of-phase limb movements, eyes-closed unresponsiveness, and pelvic thrusting (Table 1).16 Fluctuating patterns of movement and distractibility during the seizure are also suggestive of PNES.
Clinical features that may suggest psychogenic nonepileptic seizurea
No one sign is 100% specific for PNES. For instance, out-of-phase limb movements and pelvic thrusting can occur in frontal lobe epileptic seizures, without a clear ictal EEG change.
Video EEG is most helpful when there are motor signs or decreased responsiveness, but like most diagnostic tools, video EEG has limitations. For instance, if the onset of the seizure is not captured on video, postictal behavior can be confused with PNES.
Importantly, video EEG is less useful when the patient has only subjective symptoms, because epileptic aura (with purely subjective symptoms) can be scalp EEG-negative. In addition, certain epileptic seizures can be scalp EEG-negative due to movement artifact or because scalp EEG has difficulty recording from deeper areas of the brain. In these cases, referral to a comprehensive epilepsy center is recommended. As mentioned earlier, other nonepileptic events to consider are migraine, vertigo, syncope, movement disorder (eg, paroxysmal dystonia and dyskinesia), and sleep disorders such as narcolepsy, cataplexy, and parasomnias.
About 10% of patients with PNES also have epileptic seizures, so when the patient or the patient’s family describes more than 1 seizure type, it is crucial to record examples of all seizure types. Once it is confirmed that a patient has both PNES and epileptic seizures, showing the patient and family videos of the seizure types captured with video EEG, and highlighting key features of both seizure types, will help them distinguish PNES from epileptic seizures once they leave the monitoring unit.
COMMUNICATE THE DIAGNOSIS CLEARLY AND WITH EMPATHY
Presenting the diagnosis to the patient is typically the job of the neurologist who has interpreted the video EEG. Communicating the diagnosis effectively is crucial and can be therapeutic in the short term. However, if learning the diagnosis leaves the patient angry or confused, PNES and other psychiatric symptoms will likely worsen.
A survey of primary care and emergency medicine physicians found that 38% believed that episodes of PNES are intentionally produced or faked, and 63% did not feel video EEG was needed to confirm a diagnosis of PNES.17 The misperception that PNES is intentionally feigned is likely to result in mismanagement of the condition.
Many patients with PNES say the diagnosis is confusing and distressing, and they feel misunderstood, mistreated, and blamed when they seek medical care.18 About a quarter feel the diagnosing doctor does not understand their PNES symptoms.19 Receiving a diagnosis of PNES can be particularly confusing for patients who were previously diagnosed with epilepsy and treated for years with antiseizure medications.20 When their diagnosis is changed from epilepsy to PNES, patients find the news distressing because they perceive the burden of recovery is shifted from the doctor’s shoulders to theirs.21 Misperceptions about PNES and poor physician-patient communication certainly add to the emotional struggles of patients and can lead to resistance to mental health recommendations.
Since many people with PNES have a history of trauma and abuse, perceived or actual mistreatment by medical providers (via poor communication of the diagnosis) can traumatize them yet again and makes it more likely they will reject the diagnosis. Various communication strategies have been proposed, but the most important component is to deliver the diagnosis with empathy and clarity.
Key points in discussing the diagnosis with the patient are to acknowledge that their symptoms are real and can be frightening and disabling. It can be reassuring to know that they are not alone and that PNES is a diagnosis that is common in epilepsy monitoring units.
The discussion should also clarify that the patient does not have epilepsy and does not need antiseizure medications (assuming the patient does not have comorbid epileptic seizures). Rapid titration off antiseizure medications at the time of diagnosis is associated with better outcome than with delayed titration.22
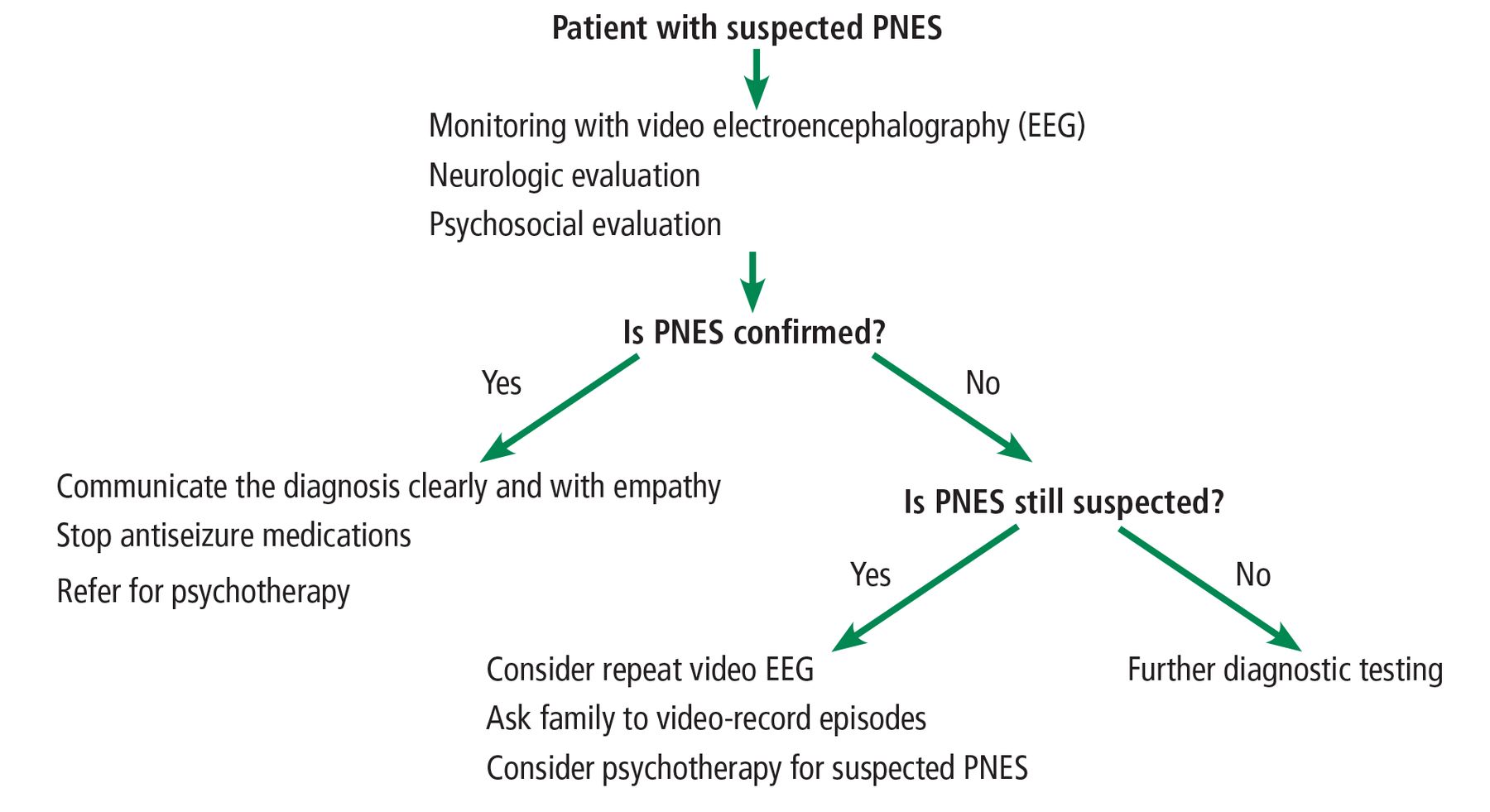
It is helpful to discuss the role of emotions and stress in producing physical symptoms, similar to the way anxiety can cause abdominal pain or headaches. Finally, it is essential to let the patient know that with treatment PNES can resolve, and that seizure control with a return to normal function should be the goal. These steps are summarized in Figure 1.
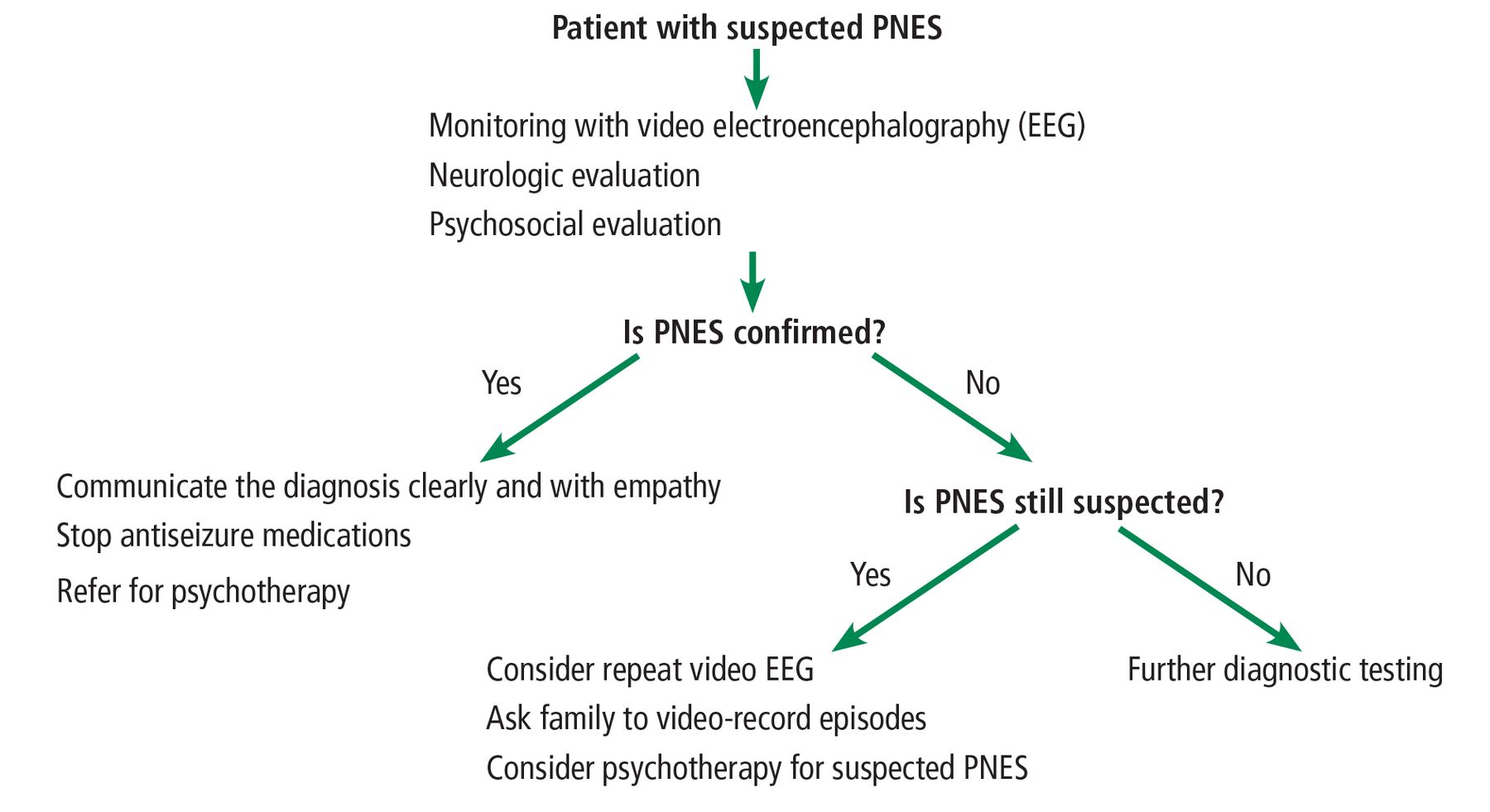
Algorithm for diagnosing psychogenic nonepileptic seizure (PNES).
TREATMENT
Emergency management
The basics of emergency medical care apply in people having a known or suspected PNES episode, as follows:
Monitor airways, breathing, and circulation
Provide for patient safety and comfort
Avoid employing noxious stimuli (eg, sternal rub) in an attempt to test responsiveness
Remain calm and reassuring
Stay with the patient until symptoms start to improve.
If the PNES diagnosis is clear from a previous video EEG evaluation and if the situation allows, encouraging the patient to engage in deep breathing can help to lessen the intensity of the episode. Once the episode has resolved, prompting the patient to identify potential triggers for the episode can be instructive and ultimately empowering.
If the seizure diagnosis is not clear, PNES should still be considered, if only briefly, before initiating escalating doses of antiseizure medications in an emergency setting.
Predisposing, precipitating, and perpetuating factors
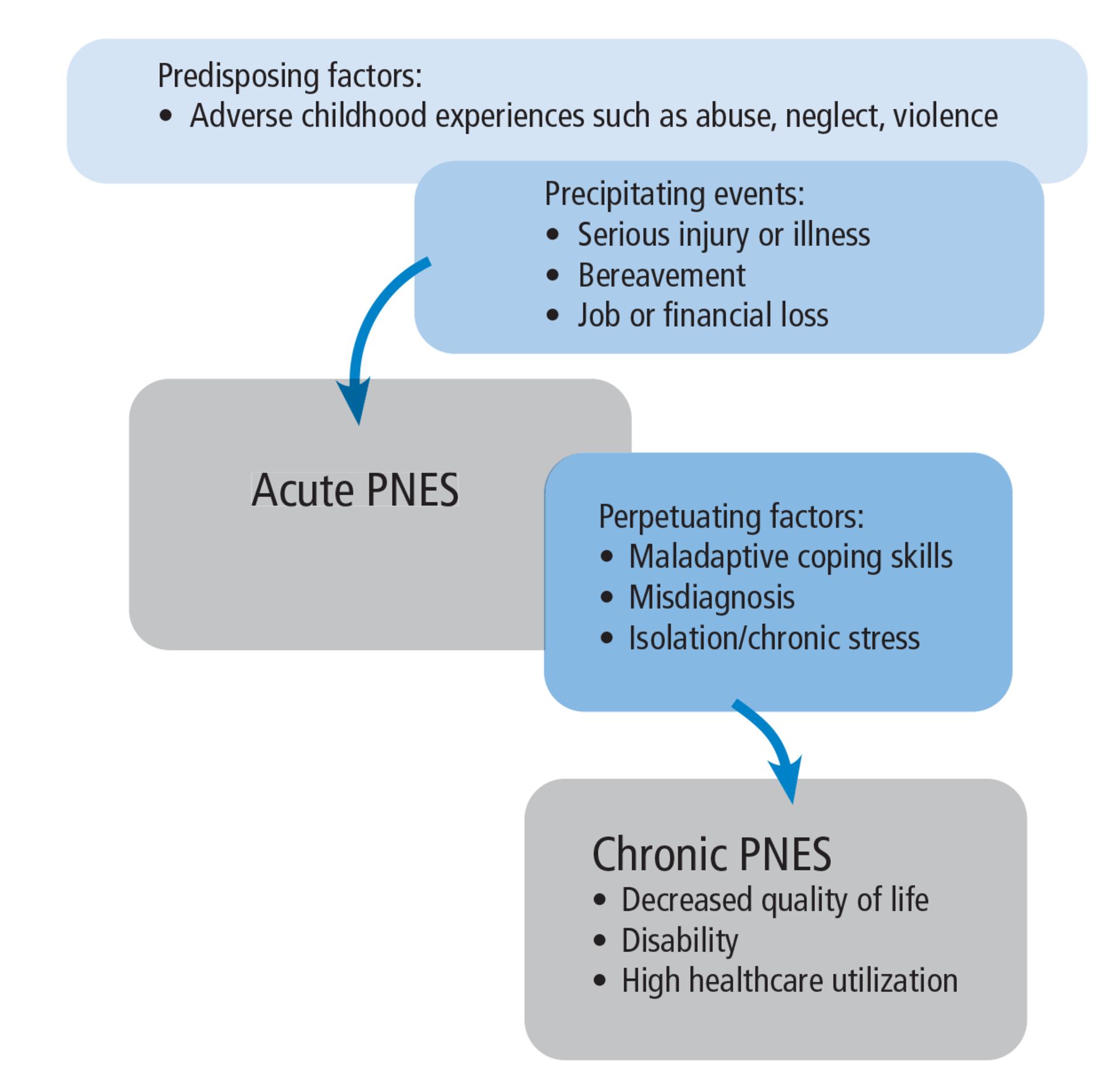
Biologic, psychological, and social factors all contribute in a complex way to predisposing patients to PNES, precipitating episodes, and perpetuating the condition, thus making it chronic (Figure 2).
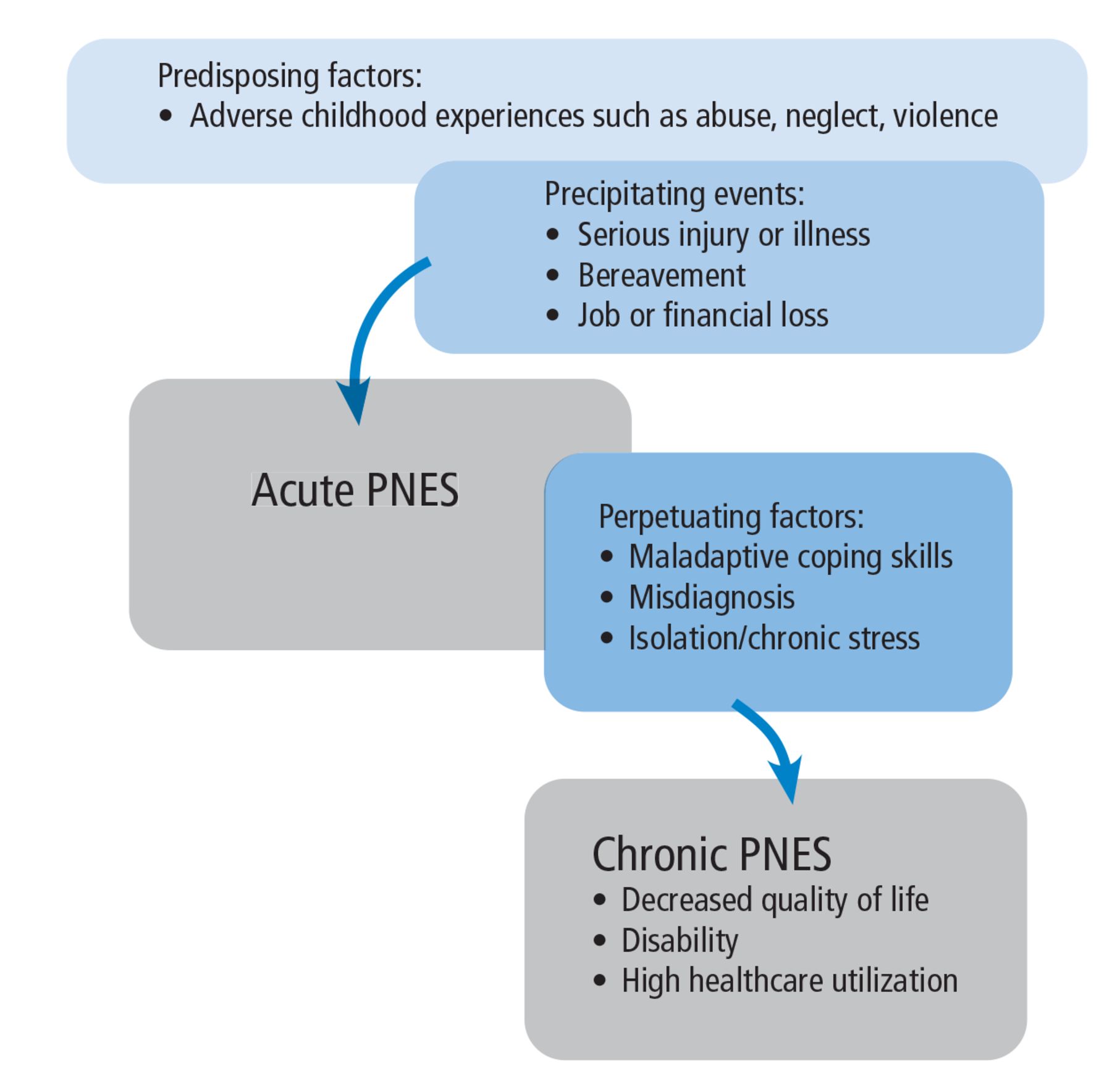
A variety of predisposing, precipitating, and perpetuating factors contribute to psychogenic nonepileptic seizure (PNES). Patients with PNES typically have multiple contributing factors.
Biologic factors include a history of head injury and of somatic conditions such as migraine, asthma, irritable bowel syndrome, chronic pain, and insomnia.
Psychological factors associated with PNES include mood disorder, anxiety, PTSD, and maladaptive coping styles. Exposure to trauma early in life can contribute to the emergence of psychiatric symptoms such as somatic dissociation due to inability to regulate emotions and cope with distress. Maladaptive coping styles, particularly the avoidant coping style and alexithymia (inability to identify and describe emotions), can make people susceptible to develop somatic symptoms as a means to release tension. Heightened somatic hypervigilance, excessive symptom preoccupation, and learned somatization can all contribute to the development of PNES.23,24
Social factors include a history of abuse, chronic stress, drug use, family dysfunction, marital discord, and financial instability.
A single factor can play multiple roles, both predisposing to and perpetuating PNES. Typically, a combination of biopsychosocial factors including physiological susceptibility, early-life trauma, maladaptive response to psychological distress, and ongoing social stressors can lead to the development and chronicity of PNES.25
Psychiatric disorders: Cause or comorbidity?
Symptoms of PNES are considered maladaptive defense mechanisms that develop in response to an underlying psychiatric disorder.26 Therefore, coexistent psychiatric disorders can be understood as causes of PNES rather than comorbidities. This relationship can be bidirectional, with psychiatric symptoms contributing to the emergence of PNES, and the struggle with PNES exacerbating existing psychiatric disorders. Therefore, the assessment and treatment of PNES should include identifying and addressing coexisting psychiatric disorders along with the PNES symptoms.
Common psychiatric comorbidities in patients with PNES include the following27:
PTSD (35%–49%)
Depressive disorders (57%–85%)
Dissociation (22%–91%)
Other somatoform disorders (22%–84%)
Axis II (personality) disorders (10%–86%).
Suicidal ideation is common in individuals with PNES, with 39% acknowledging suicidal ideation and 20% reporting suicide attempts in 1 study.28 Panic attacks, history of trauma, and history of sexual and physical abuse are also highly prevalent.
The high prevalence of trauma exposure and psychiatric comorbidity reflects the extreme vulnerability and psychological distress that patients with PNES suffer and helps explain the critical need for psychological support. A misperception of the condition as consciously feigned slights the patient’s struggle, increases distress, and worsens PNES symptoms.
Psychotherapy is effective
PNES is treatable, as demonstrated by 2 pilot randomized controlled trials of 12-session courses of cognitive behavioral therapy (CBT).29,30 A meta-analysis of psychological interventions including CBT found that 47% of patients with PNES became seizure-free, and 82% showed a reduction in seizures of at least 50%.31 PNES-tailored counseling interventions, particularly CBT-based, also improve health-related quality of life and psychosocial functioning.32
PNES-specific counseling interventions often include education about types of seizures, identifying and managing common seizure triggers, aura interruption methods, and improved emotion management skills using relaxation training and other CBT techniques.29
As mentioned earlier, controlling underlying psychiatric symptoms is an important part of treating PNES. In the case of ongoing psychiatric symptoms such as PTSD, various evidence-based psychotherapy interventions can be used concurrently or subsequently, including the following:
Hypnosis
Eye movement desensitization and reprocessing
Prolonged exposure therapy for patients with coexisting PTSD symptoms33
Cognitive processing therapy
Intensive outpatient programs for mood disorders
Dialectical behavioral therapy for patients with severe personality disorders34
Family therapy, often incorporated in individual counseling because of the high prevalence of family dynamic stress in patients with PNES.35
Pharmacologic therapy for some
Although counseling is the best intervention, antidepressants are often used to treat PNES, particularly in patients with low psychological insight or poor engagement with counseling for other reasons.29–32 There is some evidence that antidepressants alone,36 as well as antidepressants with counseling,29 can result in reduction of PNES episodes.
The benefit from benzodiazepines is mixed. Although some patients may benefit from benzodiazepines for anxiety, clobazam and clonazepam have been associated with behavioral side effects that can mimic PNES.37
Stop antiseizure medications
Continuing antiseizure medications in patients with PNES has been associated with poor outcome.38 When the diagnosis of PNES is clear, antiseizure medications should be stopped unless they are being used to manage comorbid epilepsy, chronic pain, migraine, or mood instability.
IMPROVING TREATMENT ADHERENCE
Effective treatments are available for PNES, but challenges remain, especially lack of access to treatment and patient rejection of both the diagnosis and treatment.
High attrition and poor treatment engagement are known challenges in the treatment of PNES. Predictors of poor treatment adherence include insufficient understanding of the diagnosis, unemployment, and severe psychiatric and personality disorders.28,39 Communicating the diagnosis without sufficient explanation or a clear treatment path rarely produces a good outcome, whereas patients who are given sufficient time and education about the diagnosis, as well as psychiatric support, show better outcomes.40,41
Although physicians have no control over the patient factors that predict poor treatment engagement, they do have control over how they explain the diagnosis, which in turn can affect the patient’s acceptance of the diagnosis, which is the first step in treatment engagement. Introducing the diagnosis may initially invoke intense emotions in patients, but taking sufficient time to explain PNES and answer questions, using an empathic approach to validate patients’ reactions, can help ease patient distress. Recognizing that shame and embarrassment are common reactions in these situations, a dignified and respectful conversation during the delivery of the PNES diagnosis can help the patient to be receptive of the physician’s recommendations.
The psychological approach known as motivational interviewing, often used to engage treatment-resistant patients, was shown in a randomized control trial to improve patients’ acceptance of the diagnosis, adherence to treatment, and quality of life, as well as to reduce the frequency of PNES episodes.42 Empathic and clear communication of the diagnosis and allowing sufficient time to address all of the patient’s concerns and questions are critical components of the treatment of PNES.
MORE ABOUT OUR PATIENT
We talked to the patient further and found that he began to have depressive symptoms after his grandmother died, 4 years before the onset of his seizures. In the year after her death, he began to drink alcohol and abuse drugs.
After graduating from high school in May 2020, he joined the military, but soon after, he tested positive for COVID-19 and was placed in quarantine. Being diagnosed with COVID-19 early in the pandemic when there was so little information available was a traumatic experience for him. He felt helpless and had severe crying spells because he thought he was going to die. His quarantine “buddies” were likewise experiencing depressive symptoms, and he witnessed multiple episodes of self-injurious behavior among the other recruits. While in quarantine, he developed seizures and was hospitalized.
He was eventually discharged from the military and returned home. He then enrolled in college, where he struggled with his classes and had a series of failed romantic relationships.
In the epilepsy monitoring unit, he was diagnosed with anxiety in addition to PNES. The diagnosis of PNES was explained in the context of his recent stressors, and though he was tearful, he said he felt relieved to know he did not have epilepsy. He and his family understood and accepted the PNES diagnosis, and outpatient psychotherapy was scheduled.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}