


Article Figures & Data
Figures
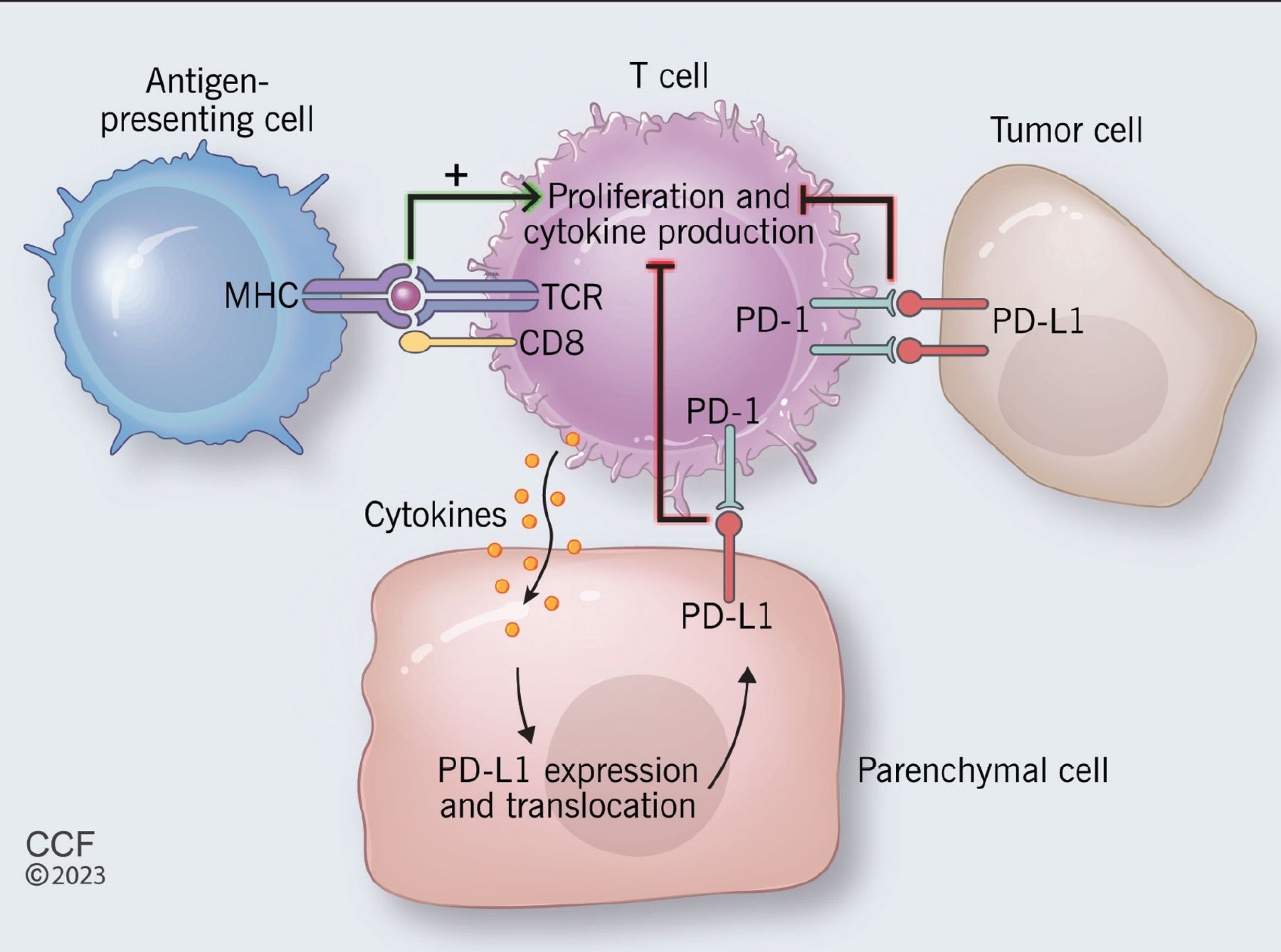
- Figure 1
Proposed mechanism of the programmed cell death protein 1 (PD-1) and programmed cell death ligand 1 pathway (PD-L1). (MHC = major histocompatibility complex ; TCR = T-cell receptor.)

Tables
Grade 1 Grade 2 Grade 3 Grade 4 Grade 5 Asymptomatic or mild symptoms or change in affected chronic condition from baseline (eg, diabetes mellitus) Moderate symptoms; limiting age-appropriate instrumental activities of daily living Severe or medically significant but not immediately life threatening; hospitalization or prolongation of existing hospitalization indicated; limiting self-care activities of daily living Life-threatening consequences; urgent intervention indicated Death Adapted from reference 18.
- TABLE 2
Thyroid dysfunction due to immune checkpoint inhibitors: American Society of Clinical Oncology guideline
Situation Action Screening Thyroid function tests, ie, thyroid-stimulating hormone (TSH) with or without thyroxine (T4) every 4–6 weeks while on therapy Asymptomatic hypothyroidism (grade 1), TSH > 4.5 and < 10 mIU/L Monitor thyroid function tests routinely as above
Continue immune checkpoint inhibitorSymptomatic hypothyroidism (grade 2) or TSH persistently > 10 mIU/L Start levothyroxine (1.6 μg/kg/day if age < 70; 25–50 μg/day if age > 70 or multiple comorbidities); monitor TSH every 6–8 weeks until TSH is at goal, then every 6–12 months unless symptoms change
Consider holding immune checkpoint inhibitor until symptoms resolve
Consider endocrine consultation for challenging presentation or for hormonal therapySeverely symptomatic hypothyroidism (grade 3 or 4) Hold immune checkpoint inhibitor until symptoms resolve
Hospital admission usually required
Endocrine consultation recommended to assist with rapid hormone replacement
Hydrocortisone should be given in the event central hypothyroidism is considered
Start on chronic levothyroxine therapy and monitor as above on discharge.Asymptomatic or mildly symptomatic thyrotoxicosis (grade 1) Continue immune checkpoint inhibitor
Start beta-blocker
Monitor TSH and T4 every 2–3 weeks after diagnosis for possible hypothyroidism transition (and treat as for primary hypothyroidism)
Consider endocrine consult for persistent thyrotoxicosis (> 6 weeks)Mildly symptomatic thyrotoxicosis (grade 2) Consider holding immune checkpoint inhibitor until symptoms improve
Consider endocrine consultation
Start on beta-blockers
Refer to endocrinologist for persistent thyrotoxicosis (> 6 weeks) for additional workup and possible medical thyroid suppressionSeverely symptomatic thyrotoxicosis (grade 3 or 4) Hold immune checkpoint inhibitor until symptoms resolve
Endocrine consult for all patients
Start on beta-blocker
Hospitalization with endocrine consultation to be considered in severe cases to guide medical therapyAdapted from reference 49.
- TABLE 3
Hypopituitarism due to immune checkpoint inhibitors: American Society of Clinical Oncology guideline
Situation Action Screening and workup Routine thyroid function tests as outlined in Table 2
If central hypothyroidism is suspected, evaluate morning adrenocorticotropic hormone (ACTH) and cortisol as well as electrolytes
ACTH stimulation testing can be falsely negative early in hypophysitis, as adrenal reserve declines slowly after pituitary stimulation is lostAsymptomatic or mild symptoms (grade 1) Consider holding immune checkpoint inhibitor until patient is stabilized on hormone replacement
Endocrine consultation
Initiate hormonal replacement for affected axis
Adrenal insufficiency: corticosteroid replacement (hydrocortisone 15–20 mg in divided doses)
No adrenal insufficiency: consider lower steroid dosing (average daily dosing over 2 months < 7.5 mg) due to report of reduced survival on higher dosing
Initiate other hormone replacement after steroid initiation and only after adrenal insufficiency is corrected, to avoid crisisModerate symptoms (grade 2) Consider holding immune checkpoint inhibitor until the patient is stabilized on hormone replacement
Endocrine consultation
Consider oral pulse-dose steroid therapy in patients with magnetic resonance imaging evidence of swelling or threatened optic chiasm compression; taper over 1 to 2 weeks, then maintenance steroid therapy
Other hormonal replacement therapy as aboveSevere symptoms (grade 3 or 4) Hold immune checkpoint inhibitor until patient is stabilized on hormone replacement
Endocrine consultation
Hospitalize or refer to emergency department for normal saline (at least 2 L) and monitored free water replacement if the patient has diabetes insipidus
Intravenous stress steroids (initial dosing: hydrocortisone 50–100 mg every 6 hours), then oral pulse-dose therapy tapered over 1–2 weeks in patients with magnetic resonance imaging evidence of significant swelling, optic chiasm compression, severe headache, or visual changes
Taper stress-dose steroids to oral maintenance dose over 5–7 days
Other maintenance therapy as above
Patients should have a medical alert device as well as education on stress-dosing for sick days, when to seek medical attention for impending adrenal crisis, and use of emergency steroid injectablesAdapted from reference 49.
- TABLE 4
Adrenal dysfunction due to immune checkpoint inhibitors: American Society of Clinical Oncology guideline
Situation Action Screening and workup No screening recommended
Workup for suspected adrenal insufficiency includes morning adrenocorticotropic hormone (> 2 times the upper limit of normal), cortisol (< 3 μg/dL), basic metabolic panel, renin, and aldosterone
Adrenocorticotropic hormone testing can be considered for indeterminate results
Rule out other causes such as infection or metastatic diseaseAsymptomatic or mild symptoms (grade 1) Consider holding the immune checkpoint inhibitor until the patient is stabilized on hormone replacement
Endocrine consultation
Start hydrocortisone treatment (15–20 mg in divided doses) and titrate to maximum 30 mg/day for residual adrenal insufficiency
Most primary adrenal insufficiency cases will also require fludrocortisone (starting dose 0.1–0.5 mg/day)
Patients should have a medical alert device as well as education on stress-dosing for sick days, when to seek medical attention for impending adrenal crisis, and use of emergency steroid injectablesModerate symptoms (grade 2) Consider holding immune checkpoint inhibitor until the patient is stabilized on hormonal replacement
Endocrine consultation
Initiate outpatient corticosteroid treatment 2–3 times the maintenance dose (hydrocortisone 30–50 mg/day; prednisone 20 mg/day) to manage acute symptoms and decrease stress dosing after 2 days
Initiate fludrocortisone as above
Patient education as aboveSevere symptoms (grade 3 or 4) Hold the immune checkpoint inhibitor until the patient is stabilized on hormonal replacement
Endocrine consultation
For inpatient management, normal saline (at least 2 L) with intravenous stress-dose steroids (initial dosing: hydrocortisone 50–100 mg every 6 hours), then taper to oral maintenance doses over 5–7 days
Maintenance therapy as above
Patient education as aboveAdapted from reference 49.
- TABLE 5
Diabetes due to immune checkpoint inhibitors: American Society of Clinical Oncology guideline
Situation Action Screening and workup Screening glucose at baseline and with each treatment cycle while on therapy and at follow-up visits for at least 6 months
Monitor symptoms for hyperglycemia
Other laboratory tests include urine or serum ketones (or both), anion gap on a metabolic panel, anti-glutamic acid decarboxylase antibody, anti-islet cell antibodies, C-peptideAsymptomatic or mild symptoms (grade 1), or type 2 diabetes with fasting glucose < 160 mg/dL and no new evidence of ketoacidosis or pancreatic autoimmunity Can continue immune checkpoint inhibitor with close clinical follow-up
Refer to primary care physician for diabetes managementModerate symptoms (grade 2), or type 2 diabetes with fasting glucose > 160–250 mg/dL and no new evidence of ketoacidosis or pancreatic autoimmunity May hold immune checkpoint inhibitor until glucose control is obtained
Urgent endocrine consultation for any patient with new-onset checkpoint inhibitor-associated diabetes
Initiate insulin
Refer to emergency department if unable to initiate therapy or if urgent outpatient specialist evaluation is unavailableSevere symptoms (grade 3 or 4), or worsening glucose, glucose > 500 mg/dL, ketoacidosis, or other metabolic abnormality Hold immune checkpoint inhibitor until glucose control is obtained to levels and symptoms similar to grade 1
Admit for diabetic ketoacidosis, volume and electrolyte resuscitation, and insulin initiation
Endocrine consultation recommended for all patients
Insulin therapy appropriate for all patientsAdapted from reference 49.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.