


Article Figures & Data
Figures
- Figure 1
Posterior-anterior chest radiography showed a widened mediastinum (yellow arrow) and right unilateral pleural effusion (red arrow).
- Figure 2
Computed tomography of the chest with contrast showed atelectasis of the right upper and middle lobes secondary to extrinsic compression of the right mainstem by mediastinal lymphadenopathy (yellow arrow) and right unilateral pleural effusion (red arrow).
- Figure 3
Green pleural fluid.
- Figure 4
Pictograph of the whole lymph node illustrating the complete effacement of the normal lymph node architecture by atypical polymorphous infiltrates.
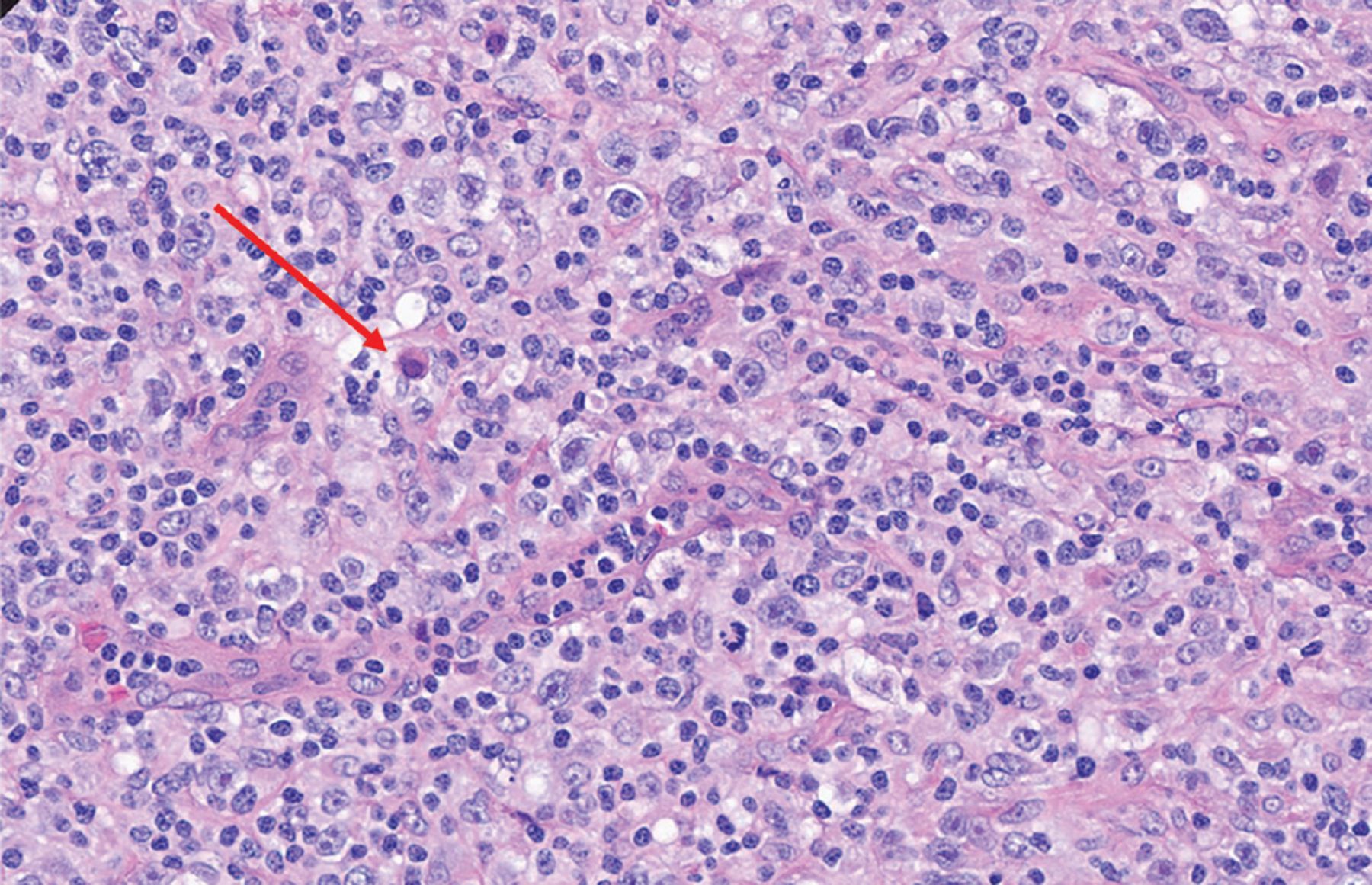
- Figure 5
The characteristic Reed-Sternberg cell (red arrow) on excisional lymph node biopsy study (hematoxylin and eosin, magnification × 40).





Tables
Diagnosis Risk factors Clinical presentation Physical examination findings Laboratory and imaging characteristics Alternative diagnosis Decompensated heart failure History of ischemic or nonischemic cardiomyopathy, heart failure Exertional dyspnea, dyspnea at rest, orthopnea, PND Elevated JVD, pedal edema, crackles on lung auscultation Transudative pleural effusion; usually bilateral simple pleural effusion Lack of prior diagnosis of heart failure, orthopnea, PND Malignancy (solid-organ or hematopoietic) Known malignancy of lungs, metastasis to the lung B symptoms (fatigue, weight loss, anorexia, night sweats, chills, fevers) Lymph node enlargement Exudative effusion; unilateral simple pleural effusion Lack of personal or family history of malignancy; lack of risk factors such as smoking Infection Immunocompromised status Fever, chills, productive cough, sweating Bronchial breaths sound on auscultation Exudative effusion; consolidation associated with parapneumonic effusion; loculated effusion; empyema; ground-glass opacities or lobular consolidation on chest CT Symptoms for a few weeks, no documented fevers Pulmonary embolism History of venous thromboembolism, active malignancy, hypercoagulable state Pleuritic chest pain Sinus tachycardia Exudative effusion; normal chest radiograph; filling defect on chest CT with contrast; may be associated with small pleural effusion No known risk factors for venous thromboembolism; large pleural effusion Lymphangioleiomyomatosis Young females in reproductive age group Chronic dyspnea, fatigue, spontaneous pneumothorax, pleural effusions Associated with axillary and mediastinal lymphadenopathy Chylous, exudative pleural effusion; cystic lung disease; ground-glass opacities and septal thickening on chest CT; renal angiomyolipoma Lack of history of spontaneous pneumothorax Cirrhosis Alcoholic or nonalcoholic liver disease Jaundice, ascites, fatigue, weight loss Fluid thrill, shifting dullness on abdominal examination Transudative pleural effusion; cirrhotic morphology of liver, ascites Lack of history, risk factors for liver disease Chylothorax History of thoracic surgery, trauma, congenital disorders Dyspnea, fatigue, yellow nails Decreased breath sounds at site of pleural effusion, lymphadenopathy Chylous pleural effusion; unilateral pleural effusion Lack of thoracic duct injury due to surgery, trauma CT = computed tomography; JVD = jugular venous distention; PND = paroxysmal nocturnal dyspnea
Blood cell count and differential A neutrophilic-predominant pleural effusion would make bacterial infection the most likely cause
Lymphocytic pleural effusion is mainly encountered in conditions like rheumatoid arthritis-associated pleural effusion and fungal or tuberculosis-associated pleural effusionCholesterol level Cholesterol levels > 60 mg/dL are seen in exudative pleural effusion Cytology Pathologic analysis of pleural fluid allows for detection of malignancy Culture and Gram stain Allows for the speciation of the pathogenic organism
Culture for bacteria, fungal, and acid-fast bacilli can be sent
Antimicrobial resistance can be determined by sensitivity dataAmylase level Elevated levels seen in acute pancreatitis-associated exudative pleural effusion Triglyceride level Elevated (> 110 mg/dL) in chylothorax Bilirubin level Elevated in biliothorax Albumin level Pleural fluid albumin and serum albumin gradient allow for the determination of pseudoexudative and exudative effusions in the setting of diuretic use Hematocrit Pleural fluid hematocrit > 50% is pathognomonic for hemothorax pH Low pH pleural fluid seen in empyema or rheumatoid arthritis-associated pleural effusion Light criteria Differentiates between exudative or transudative pleural effusion; if at least 1 of the following criteria is met, the pleural effusion is exudative: Ratio of pleural fluid protein to serum protein concentration > 0.5
Pleural fluid LDH greater than two-thirds of the upper limit of normal for serum LDH
Ratio of pleural fluid LDH to serum LDH concentration > 0.6
LDH = lactate dehydrogenase
Data from references 2–9.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.