


ABSTRACT
The risk of developing cervical cancer is not equal across populations—individual health history, economic, political, and societal factors influence cervical cancer risk. Certain health conditions, including human immunodeficiency virus (HIV) infection, immunosuppression, and history of high-grade cervical dysplasia, are associated with higher cervical cancer risk and warrant distinct screening, surveillance, and management guidelines. It is imperative for clinicians to recognize high-risk groups and apply appropriate corresponding guidelines. However, this can be difficult in practice, as recommendations regularly evolve. This review offers up-to-date guidance in a case-based format on cervical cancer screening, surveillance, and management for high-risk patients.
Cervical cancer screening, surveillance, and management in high-risk populations differ compared with average-risk populations.
Individuals at increased risk include those with a history of HIV infection, immunosuppression, in utero exposure to diethylstilbestrol, or high-grade cervical dysplasia or human papillomavirus–related lower genital tract cancer, and those who have been underscreened.
High-risk patients generally require more-intensive screening (ie, every 3 years vs every 5) and screening past age 65.
Cervical cancer is the fourth most common cancer in women worldwide and a leading cause of cancer deaths in developing parts of the world.1,2 In resource-rich countries, cervical cancer incidence and mortality are lower due to the availability of screening and human papillomavirus (HPV) vaccination.1 However, certain populations in the United States have a higher cervical cancer incidence, including individuals who are immunocompromised due to human immunodeficiency virus (HIV) infection3 or other causes or who are living in communities with higher poverty levels, likely due to limited access to healthcare and screening.4 Moreover, studies suggest that the proportion of US patients who are up-to-date on cervical cancer screening has decreased in recent years, from 86% in 2005 to 77% in 2019, with the lowest rates in non-White, underinsured, rural, and nonheterosexual women.5
Persistent infection with oncogenic high-risk HPV, particularly subtypes 16 and 18, causes almost all cases of cervical cancer.6,7 Fortunately, the vast majority of cervical HPV infections are transient.8,9 Risk factors for persistent HPV infection include infection with oncogenic subtypes, older age, immunosuppression, smoking, and possibly other sexually transmitted infections—although it is unclear if this is correlation or causation.7,10 When cervical HPV infection persists, progression from initial infection to cervical intraepithelial neoplasia (CIN) and finally invasive cancer takes years to decades.11 Cervical cancer screening can detect precancerous changes, and treatment of these precursors can prevent the development of invasive cancer.12
SCREENING FOR AVERAGE-RISK PATIENTS
There are 3 methods generally used for cervical cancer screening:
Cytology, or Papanicolaou (Pap) test: evaluation of cellular morphology for abnormalities
Primary HPV testing: detection of DNA from high-risk HPV with genotyping to identify whether HPV-16, HPV-18, or other high-risk genotypes are present; primary HPV testing should be ordered with reflex cytology (performed if the sample is positive for HPV)
Cotesting: cytology and high-risk HPV testing administered together.
Because cytology alone has lower sensitivity for pre-cancer and cancer than HPV-based testing (ie, primary HPV testing or cotesting),13 cytology alone should be repeated every 3 years, while HPV-based testing can be repeated every 5 years.12,13 Primary HPV testing is a more efficient screening method than cotesting but is not universally available. There are currently only 2 US Food and Drug Administration–approved primary HPV tests,12 so clinicians should ensure an approved assay is used.
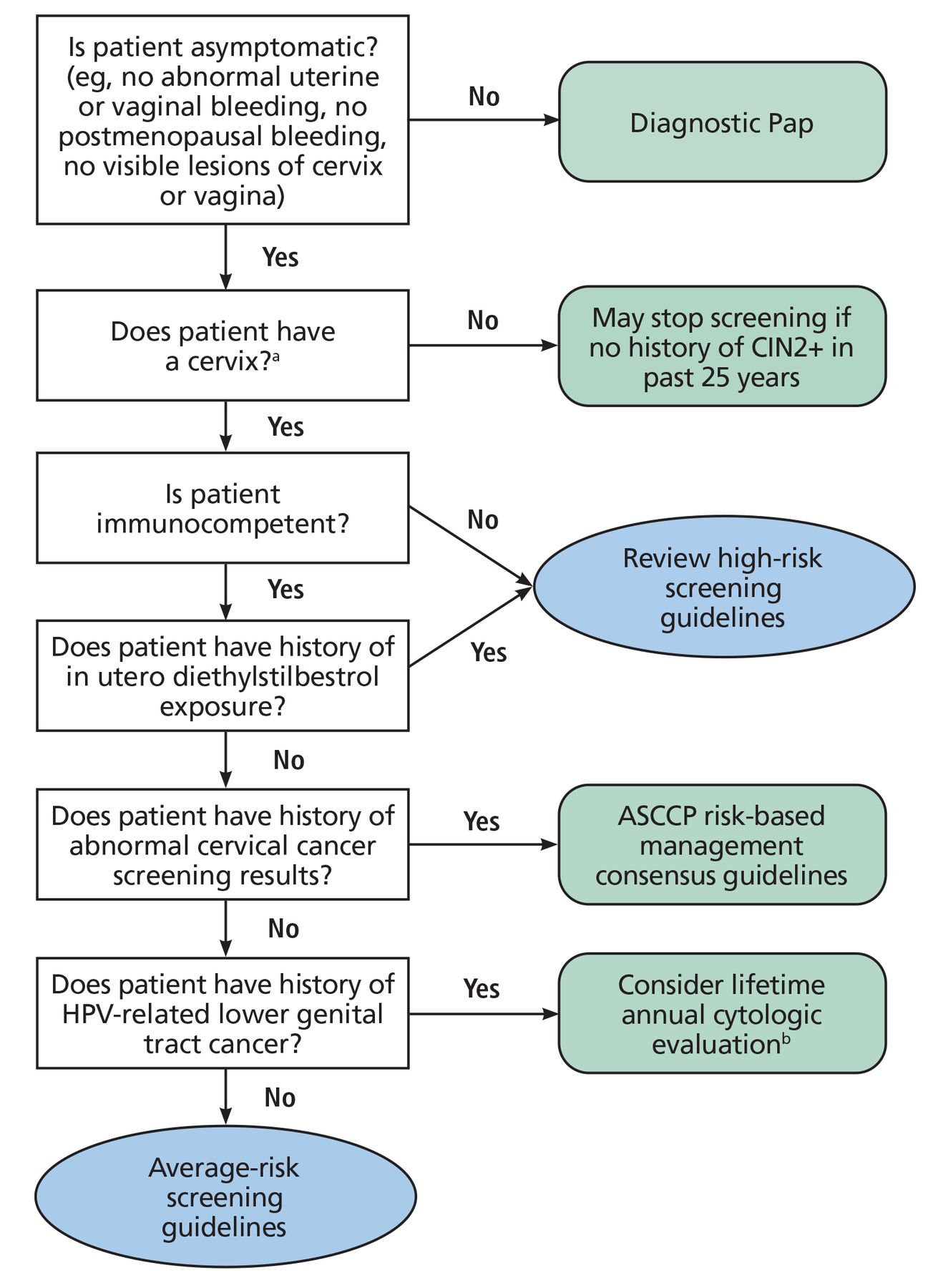
Screening recommendations for average-risk individuals vary by professional organization. We typically use either the 2018 US Preventive Services Task Force13 or 2020 American Cancer Society guidelines12 (Table 1). Figure 1 provides guidance on how to identify average-risk patients.14,15 Note that both guidelines recommend following age-specific screening recommendations for all average-risk patients, regardless of HPV-vaccination status or sexual activity.12,13
Cervical cancer screening among average-risk patients

Who can follow average-risk screening guidelines?
aFor patients who are uncertain if their cervix was removed during a benign hysterectomy, clinicians can review surgical records or perform an examination to determine the presence of the cervix.
bLifetime annual cytologic evaluation based on current Society of Gynecologic Oncology recommendations.15
ASCCP = American Society of Colposcopy and Cervical Pathology; CIN2+ = cervical intraepithelial grade 2 or higher; HPV = human papillomavirus; Pap = Papanicolaou
Based on data from reference 14.
Both the US Preventive Services Task Force and American Cancer Society guidelines note that there is no significant benefit of continuing to screen patients who are older than 65 and have had previous adequate screening with no history of CIN2, CIN3, adenocarcinoma in situ, or invasive cancer (collectively termed CIN2+) in the past 25 years (Table 2).12,13 Patients who have undergone a hysterectomy with removal of the cervix (total hysterectomy) for benign indications with no history of CIN2+ in the past 25 years can also discontinue screening. Patients who have undergone a hysterectomy that retained the cervix (subtotal or supracervical hysterectomy) should continue screening per guidelines for average- or high-risk patients, as clinically appropriate.12,13
When to stop cervical cancer screening in average-risk patients
MANAGEMENT FOR AVERAGE-RISK PATIENTS
For average-risk patients, clinicians should use the 2019 American Society of Colposcopy and Cervical Pathology (ASCCP) risk-based management consensus guidelines16 to interpret HPV and cytology results and decide on appropriate next steps. ASCCP has created a management guidelines web application (https://app.asccp.org) that is available free of charge and a smartphone application (https://www.asccp.org/mobile-app) available for purchase. These guidelines are based on the principle of “equal management for equal risk” and therefore follow a risk-based rather than a results-based approach to determine management.
Risk is estimated using current screening results and prior screening and colposcopic biopsy results (if known) while considering personal factors such as age and frequency of screening. Decisions are based on whether the immediate risk of CIN3+ (CIN3, adenocarcinoma in situ, or invasive cancer) is 4% or greater. This level of risk requires further management, which typically necessitates the involvement of gynecology or gynecology-oncology for colposcopy or treatment. If the risk is less than 4%, then the tool looks at the 5-year risk of CIN3+ to determine the surveillance interval (eg, repeat screening in 1, 3, or 5 years). These patients can continue to be followed in a primary care setting.16
SCREENING AND MANAGEMENT FOR HIGH-RISK PATIENTS: CASE SCENARIOS
The following cases illustrate commonly encountered challenges in screening and managing patients at increased risk for developing cervical cancer.
Case 1
A 35-year-old woman with a history of systemic lupus erythematosus (not currently on medication) presents for an annual examination. Her last Pap test 3 years ago was normal and negative for HPV. She asks if she needs a Pap test. Her physician advises that she can wait another 2 years because she had negative cotesting 3 years ago and is not on immunosuppressive medication.
Case 2
A 45-year-old woman who recently underwent hysterectomy presents for an annual examination. She asks if she needs a Pap test. She reports that her hysterectomy was performed for fibroids and heavy menstrual bleeding. The pathology was benign, and the report confirms the cervix was removed. She mentions having had an abnormal Pap test in her 30s requiring “a procedure” but that subsequent Pap tests were normal. Her physician advises that she does not need further cervical cancer screening because the cervix was removed.
Case 3
A 68-year-old woman with a history of hypertension presents for an annual examination. She recently relocated and is new to the clinic. While reviewing the care gaps in the electronic medical record, which generates alerts based on patient age, the physician notes that they need to discuss breast cancer screening. There is no alert for cervical cancer screening, so the physician assumes that the patient has aged out and does not need anything further at this time.
WHO IS CONSIDERED HIGH-RISK?
Individuals who have a history of HIV, solid organ or hematopoietic stem cell transplant, systemic lupus erythematosus, treatment with immunosuppressive medications, in utero diethylstilbestrol (DES) exposure, high-grade cervical dysplasia, or HPV-related lower genital tract cancer or who have been underscreened or never-screened are all at higher risk for developing invasive cervical cancer.3,10,15,17,18 As such, there are distinct screening and management recommendations for these individuals.
Cervical cancer screening recommendations for patients who are immunosuppressed but do not have HIV are limited due to a lack of quality evidence. Following a detailed literature review, Moscicki et al17 published guidelines for cervical cancer screening in immunosuppressed women without HIV infection and determined that the following patient populations being treated with immunosuppressive medications (Table 3) have a higher risk of developing cervical cancer compared with the general population:3
Solid organ transplant
Hematopoietic stem cell transplant
Systemic lupus erythematosus (regardless of treatment status)
Inflammatory bowel disease or rheumatoid arthritis.
Immunosuppressants and immunosuppressive treatments
Note that this group found that patients with systemic lupus erythematosus are at increased risk of developing cervical dysplasia and cancer regardless of treatment status.17 The underlying mechanism for this is unclear but is postulated to stem from increased risk of HPV infection owing to underlying immune dysregulation.19
SCREENING AND MANAGEMENT IN HIGH-RISK POPULATIONS
HIV infection
Cervical cancer screening guidelines for individuals living with HIV are well-supported by retrospective and prospective studies.3,14,16,20,21 Current US Department of Health and Human Services and National Institutes of Health Office of AIDS Research screening and management guidelines for individuals living with HIV are summarized in Table 4.3,16,20,21 Briefly, cervical cancer screening should begin at the time of initial HIV diagnosis but not before age 21. Cytology (Pap test) is the recommended screening method in individuals less than 30 years old and is performed annually for a total of 3 years. If the 3 consecutive Pap tests are normal, then follow-up screening is recommended every 3 years.
Cervical cancer screening and management among individuals with HIV
Individuals 30 years or older living with HIV should be screened with cytology alone using the approach detailed above or with cotesting every 3 years to continue throughout the individual’s lifetime (and not, as in the general population, end at age 65).3 Primary HPV testing is not approved for use in patients with HIV as it has not been validated in this population.
Patients with HIV are at increased risk for other HPV-associated cancers as well. At the time of cervical cancer screening, the genitalia and perianal region should be carefully examined for visual signs of warts or invasive cancer.3 If a patient with HIV undergoes a total hysterectomy for benign disease and has no history of CIN2+, then ongoing routine screening for cervical or vaginal cancer is generally not necessary. However, female patients with a history of CIN2+ are at increased risk for vaginal and vulvar cancer and should be followed with an annual vaginal cuff Pap test.3 Some providers perform more frequent screening or resume screening after hysterectomy for benign disease if HIV is poorly controlled or begins to progress (eg, rising viral load, falling CD4 level, new opportunistic infection). However, there are no current guidelines around this practice.
Individuals with HIV have a higher risk of CIN3+ with low-grade abnormalities on cytology. As such, regardless of age, colposcopy is recommended for HPV-positive atypical squamous cells of undetermined significance3,14,21 and all cytology results of low-grade squamous intraepithelial lesion or worse, regardless of HPV test results (if completed).16 Clinicians can refer to the ASCCP web or mobile application (https://www.asccp.org).16 In general, treatment for CIN in patients with HIV should be managed according to ASCCP guidelines.3,16
Immunosuppressed, no history of HIV
Immunosuppressive therapy. Per ASCCP, patients with a history of solid organ transplant or hematopoietic stem cell transplant, systemic lupus erythematosus (regardless of treatment), and inflammatory bowel disease or rheumatoid arthritis on immunosuppressive therapy should follow the US Department of Health and Human Services screening and management guidelines for individuals with HIV.3,17 Patients with inflammatory bowel disease or rheumatoid arthritis not on immunosuppressive therapy or patients with type 1 diabetes mellitus should follow screening guidelines for average-risk individuals.17 Patients who have undergone hematopoietic stem cell transplant and develop genital graft-vs-host disease or chronic genital graft-vs-host disease should resume annual cervical cytology until 3 consecutive normal results or repeat baseline cotesting (if ≥ 30 years).17
Transplant. Screening guidelines for transplant patients differ between organizations.3,17,22–25 The American Society of Transplantation recommends screening with Pap or cotesting every 6 months for the first year after solid organ transplant, then annually indefinitely if the first tests are negative, although this has been noted as a weak recommendation based on low-quality evidence.23 The American Society of Transplantation suggests changing the frequency back to every 6 months for 1 year following treatment for rejection. These same American Society of Transplantation guidelines also recommend that transplant recipients be screened with the same periodicity as women with HIV infection, in keeping with ASCCP and Moscicki et al.17 A study modeling the application of US Department of Health and Human Services screening intervals for women with HIV to solid organ transplant patients found that more than two-thirds could have safely qualified for extending screening to every 3 years after 3 consecutive annual benign cytologic test results.24 Further studies are needed among solid organ transplant recipients.
Autoimmune diseases. Notably, there are other groups of patients who are immunosuppressed, not specifically listed above, who may also warrant more intensive screening. For example, Australia’s Cancer Council cervical cancer screening guideline25 recommends considering HPV-based screening every 3 years for patients who are being treated with immunosuppressive therapy for autoimmune diseases such as neuromyelitis optica or sarcoidosis, as well as for patients with congenital immune deficiency. However, there are no definitive recommendations for patients with other autoimmune diseases, as data are limited in these populations. As such, clinicians may consider shared decision-making for patients on active immunosuppression for autoimmune diseases not specifically considered by current guidelines,17 as it may be reasonable to follow screening guidelines for individuals with HIV.3,17
History of high-grade cervical dysplasia
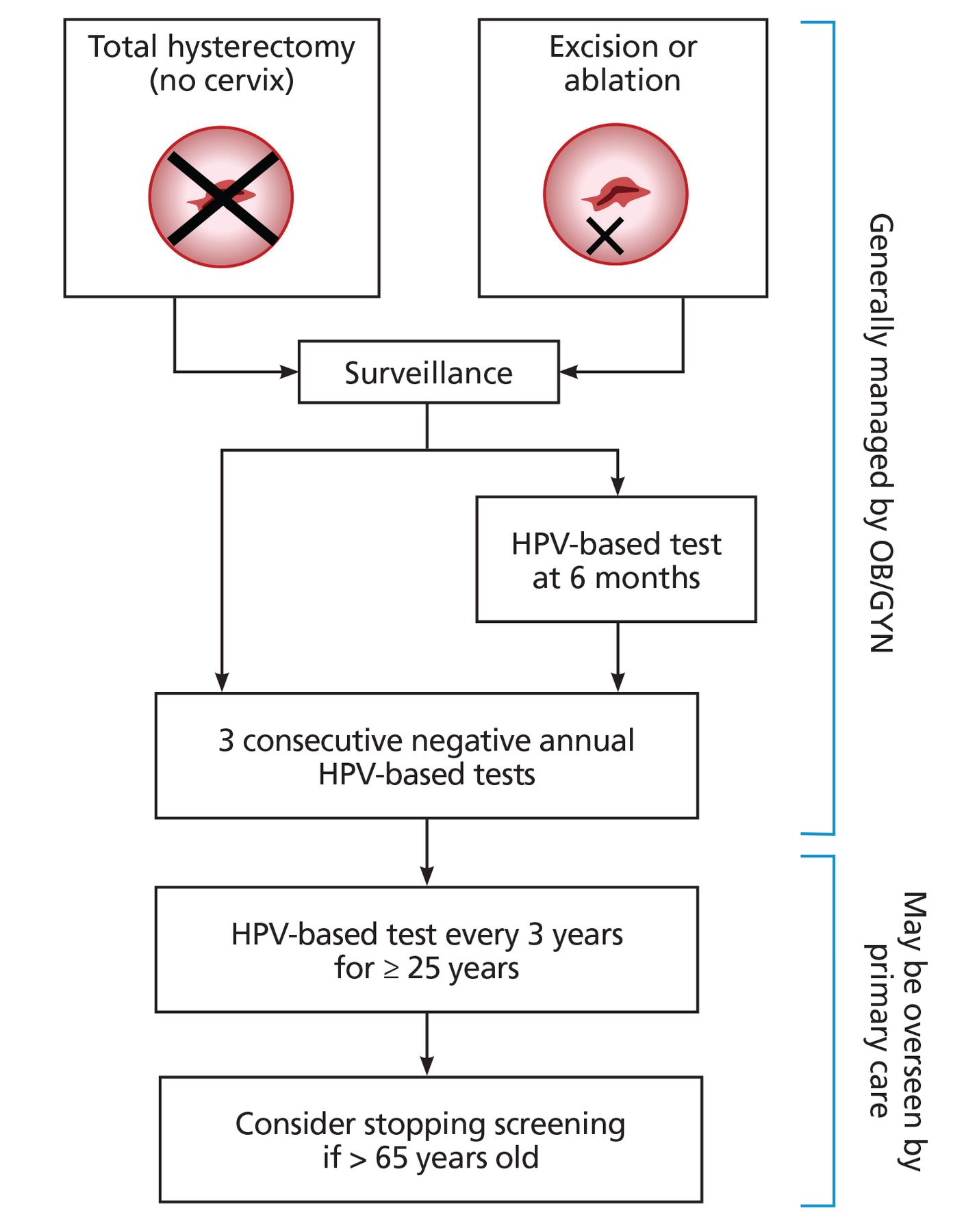
After a diagnosis with high-grade cytology or histology (ie, high-grade squamous intraepithelial lesion or CIN2, CIN3, or adenocarcinoma in situ), patients require treatment followed by increased short-term and long-term surveillance, based on the 2019 ASCCP risk-based management consensus guidelines.16 Patients treated with total hysterectomy should undergo 3 annual HPV-based tests (Figure 2). Patients treated with excision (eg, cold knife or laser conization, loop electrosurgical excision procedure) or ablation (eg, cryotherapy, carbon dioxide laser or thermal ablation), with the cervix left in place, should also receive HPV-based testing at 6 months, then annual HPV-based testing until 3 consecutive normal HPV-based tests. Then patients can enter long-term surveillance with HPV-based testing every 3 years for a minimum of 25 years, even beyond age 65. Note that these patients should never return to 5-year interval testing.

Management and surveillance for patients with a history of high-grade cervical dysplasia (high-grade squamous intraepithelial lesion, cervical intraepithelial 2 or 3, or adenocarcinoma in situ).
HPV = human papillomavirus; OB/GYN = Obstetrics and Gynecology
If a patient reaches 65 years and has completed the recommended 3-year interval screening for 25 years, then clinicians can use shared decision-making to determine the need for continued screening.16,26–28 Approximately 20% of cervical cancers occur in patients older than 65 years.16,26,29 Long-term population studies suggest a persistent 2-fold increase in cervical cancer risk after treatment of a histologic high-grade squamous intraepithelial lesion, which continues for at least 25 years and seems to be higher for patients older than 50.16,27,28 As cervical cancer risk appears to remain above general population levels,27 continued screening is acceptable, as long as the patient remains in good health. In contrast, discontinuation of screening is recommended if a patient has limited life expectancy.
HIV and cervical dysplasia. Patients with HIV and a history of a high-grade squamous intraepithelial lesion should generally undergo treatment followed by increased short-term and long-term surveillance according to ASCCP guidelines with cotesting, as primary HPV testing is not approved for patients with HIV.3,16 Surveillance should be continued throughout a patient’s lifetime, regardless of treatment choice (ie, even if treated with total hysterectomy).3 CIN recurs more frequently among patients with HIV,30 and risk of recurrence may correlate with degree of immunosuppression.21,30 As such, some clinicians perform more frequent follow-up in patients with HIV, particularly those with poorly controlled disease, although there are no current guidelines for this practice.3
History of HPV-related lower genital tract or anal cancer
Patients with HPV-associated invasive lower genital tract cancer (vulvar, vaginal, or cervical cancer) who have successfully undergone primary treatment are still at an increased risk for not only local disease recurrence but also for other HPV-related malignancies.15 Although the optimal surveillance strategy for these patients has not yet been established, the Society of Gynecologic Oncology15 recommends close monitoring by gynecologic oncology providers with complete assessment of areas susceptible to HPV-infection, including the vulva, vagina, cervix, and the perianal region, via visual inspection, speculum, bimanual, and rectovaginal examination. Although data are limited, this group also recommends lifetime annual cytologic evaluation of the cervix or vagina if the cervix is removed.
At time of diagnosis with anal cancer, it is recommended that female patients additionally undergo screening for cervical cancer if they are not up to date, given the frequent association between anorectal HPV infection and HPV infection of the cervix.31 However, there are no specific recommendations for increased frequency of cervical cancer screening in individuals who have completed primary treatment for anal cancer. At present, these individuals can follow screening guidelines for average-risk individuals.32,33
DES exposure
Before 1971, millions of people were exposed in utero to DES given to mothers to prevent pregnancy complications.18 Several adverse outcomes have been linked to this exposure, including increased risk of developing vaginal and cervical clear-cell adenocarcinoma, a rare form of cervical cancer not related to infection with high-risk HPV, as well as precursors of cervical and vaginal cancer (ie, squamous intraepithelial lesions or CIN).12,18,34 Historically, DES-exposed patients were advised to have annual pelvic examinations with visualization of the cervix and vaginal wall, and collection of cytology specimens from the cervix and all 4 quadrants of the vagina.35 However, most guidelines do not specifically address screening in patients who were exposed to DES and do not have updated recommendations to reflect the aging DES-exposed population.12,35 Moreover, there is no specific guidance on the incorporation of HPV-based testing in addition to cytology.
Palpation for focal lesions or areas of abnormal tissue growth is a crucial part of the examination for DES-exposed patients and may provide the only evidence of clear-cell adenocarcinoma.36 During inspection, the speculum should be gently rotated as it is withdrawn to fully assess the entire vaginal wall. Colposcopy is no longer recommended as part of routine screening but should be used to follow-up any abnormal cytology.35 When abnormal cytology is reported, it may be helpful to consult a gynecologist experienced in evaluating DES-exposed patients, when available. There are no clear recommendations for when to stop screening; however, it may be reasonable to continue annual screening as long as the patient would be interested in treatment should cancer be detected.35
Inadequate prior screening
The majority of invasive cervical cancer cases occur in individuals who were inadequately screened, never screened, or were unable to complete appropriate follow-up and treatment.10,12,13 Moreover, in the United States, cervical cancer incidence and mortality are disproportionately high among racial and ethnic minorities (eg, African American, American Indian and Alaska Native, Hispanic, Asian American), sexual and gender minorities, individuals with disabilities, recent immigrants, individuals with low income, the uninsured and underinsured, medically underserved patients, and geographically isolated populations with limited access to care. Targeted outreach to select populations may help address these disparities.
One other promising possible solution is HPV self-sampling.37 Self-sampling was recently approved by the US Food and Drug Administration for use in the healthcare setting and may help increase screening of women who have traditionally faced barriers to care or have experienced trauma.12,38,39
Note that in patients who have never been screened or have rarely been screened (defined by ASCCP as patients who have not undergone screening within the past 5 years) and who are not pregnant and are 25 or older, expedited treatment (ie, treatment without preceding colposcopic biopsy) should be considered for HPV-positive high-grade squamous intraepithelial lesion cytology, regardless of HPV genotype.16
When caring for older patients with inadequate prior screening, it may be reasonable to order cotesting to establish a new “baseline” rather than primary HPV testing or cytology alone. Cervical cancer screening should be continued beyond age 65 in patients who have not had adequate prior screening (Table 2) or have an unknown screening history.13 Inadequate screening at younger ages or stopping screening before criteria for cessation have been met are important risk factors for developing cervical cancer at older ages and being diagnosed with more advanced stage disease.12 In the absence of a history or confirmation of recent adequate negative screening results, clinicians should continue screening patients beyond age 65 if their life expectancy is more than 10 years, at least until criteria for cessation are confirmed or longer, based on shared decision-making.
CASES REVISITED
Case 1
A 35-year-old woman with systemic lupus erythematosus, regardless of treatment status, is at elevated risk for developing invasive cervical cancer and therefore should follow US Department of Health and Human Services screening guidelines for individuals with HIV.3,17 She should undergo screening with cotesting every 3 years and therefore is due for screening now. Note that cytology alone would also be an option but would require clarifying whether she had previously completed 3 consecutive annual Pap tests with normal results.
Case 2
A 45-year-old woman who has had a hysterectomy should be evaluated for type of hysterectomy performed (ie, with or without removal of cervix) and history of CIN2+ in the past 25 years. Removal of the cervix can be confirmed by reviewing the hysterectomy operative or pathology reports or by examination with speculum and palpation. A history of CIN2+ can be ascertained by reviewing prior pathology reports, or when needed, by eliciting further history on prior procedures, as loop electrosurgical excision procedures or cone procedures are typically performed for higher grade (eg, ≥ CIN2 or high-grade squamous intraepithelial lesion) colposcopic biopsy results.
For this patient, if a history of CIN2+ is confirmed, she will need long-term surveillance with HPV-based testing of the vaginal cuff at 3-year intervals for a minimum of 25 years from date of the loop electrosurgical excision procedure or cone procedure (even if the patient were to turn 65 during that period), even though her cervix has now been removed. Again, note that this patient should never return to screening every 5 years.
Case 3
A 68-year-old woman should be evaluated to determine whether she is at average or high risk for developing cervical cancer (eg, history of immunosuppression or history of CIN2+ in the past 25 years), the presence or absence of a cervix, and adequacy of prior screening. Adequate prior screening for this patient is defined as 3 consecutive negative cytology screenings or tests in the previous 10 years with the most recent having been within 3 years, or 2 consecutive negative HPV-based tests in the previous 10 years with most recent having been within 5 years. It can be difficult, particularly when patients relocate or transfer from a different healthcare system, to obtain documentation of screening history. However, the physician should attempt to review this history with the patient, send record-release requests, and, in the absence of confirmation, consider continued screening until criteria for cessation of screening are met.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.
![]()
Clicking the link below will connect you to begin the credit-claiming process for CME and MOC. After clicking on the link, scroll to the bottom of the page and click on “Complete the CME/MOC Process.” You will need your myCME login information to access this.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.