


Article Figures & Data
Figures
- Figure 1
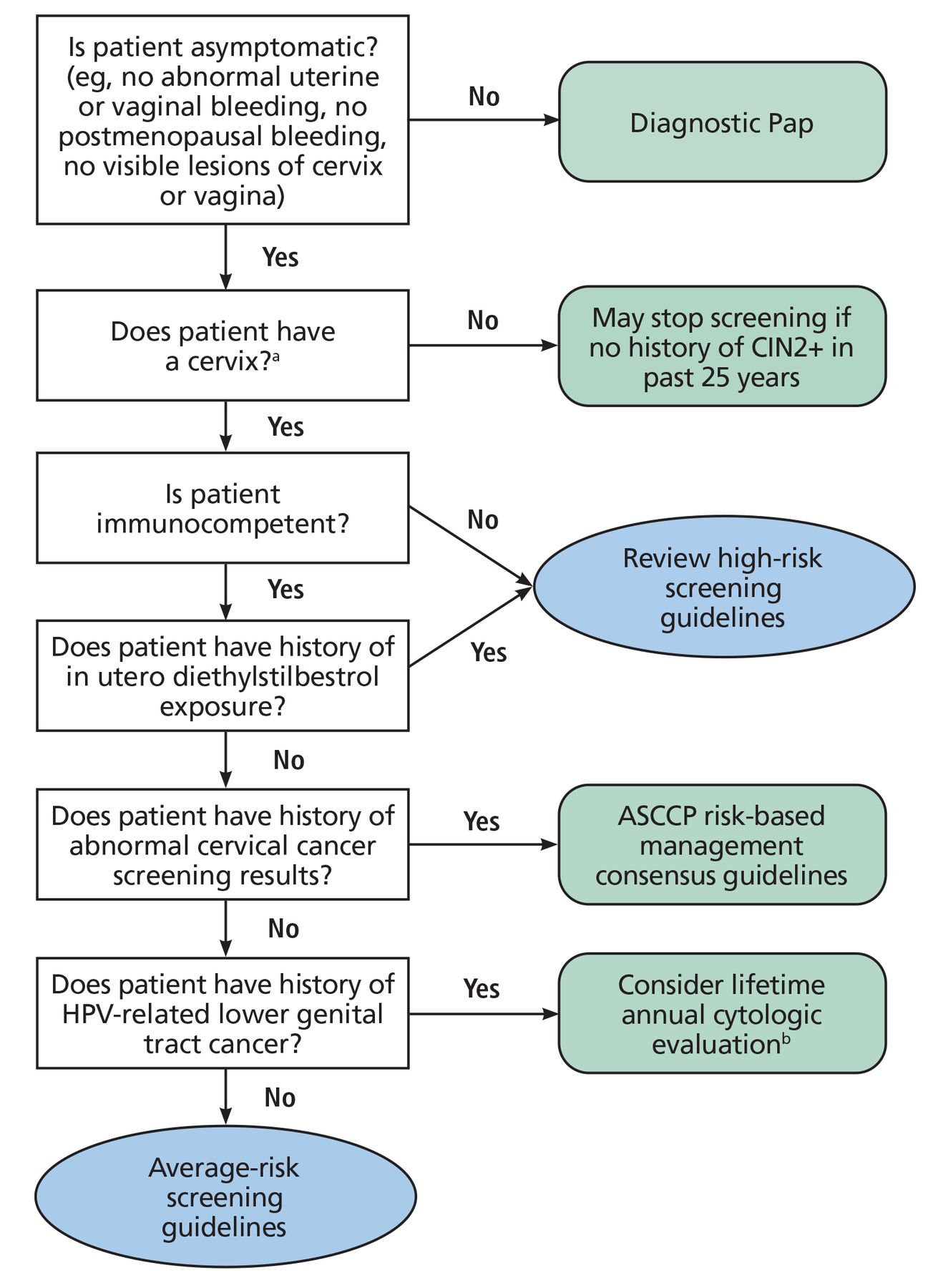
Who can follow average-risk screening guidelines?
aFor patients who are uncertain if their cervix was removed during a benign hysterectomy, clinicians can review surgical records or perform an examination to determine the presence of the cervix.
bLifetime annual cytologic evaluation based on current Society of Gynecologic Oncology recommendations.15
ASCCP = American Society of Colposcopy and Cervical Pathology; CIN2+ = cervical intraepithelial grade 2 or higher; HPV = human papillomavirus; Pap = Papanicolaou
Based on data from reference 14.
- Figure 2
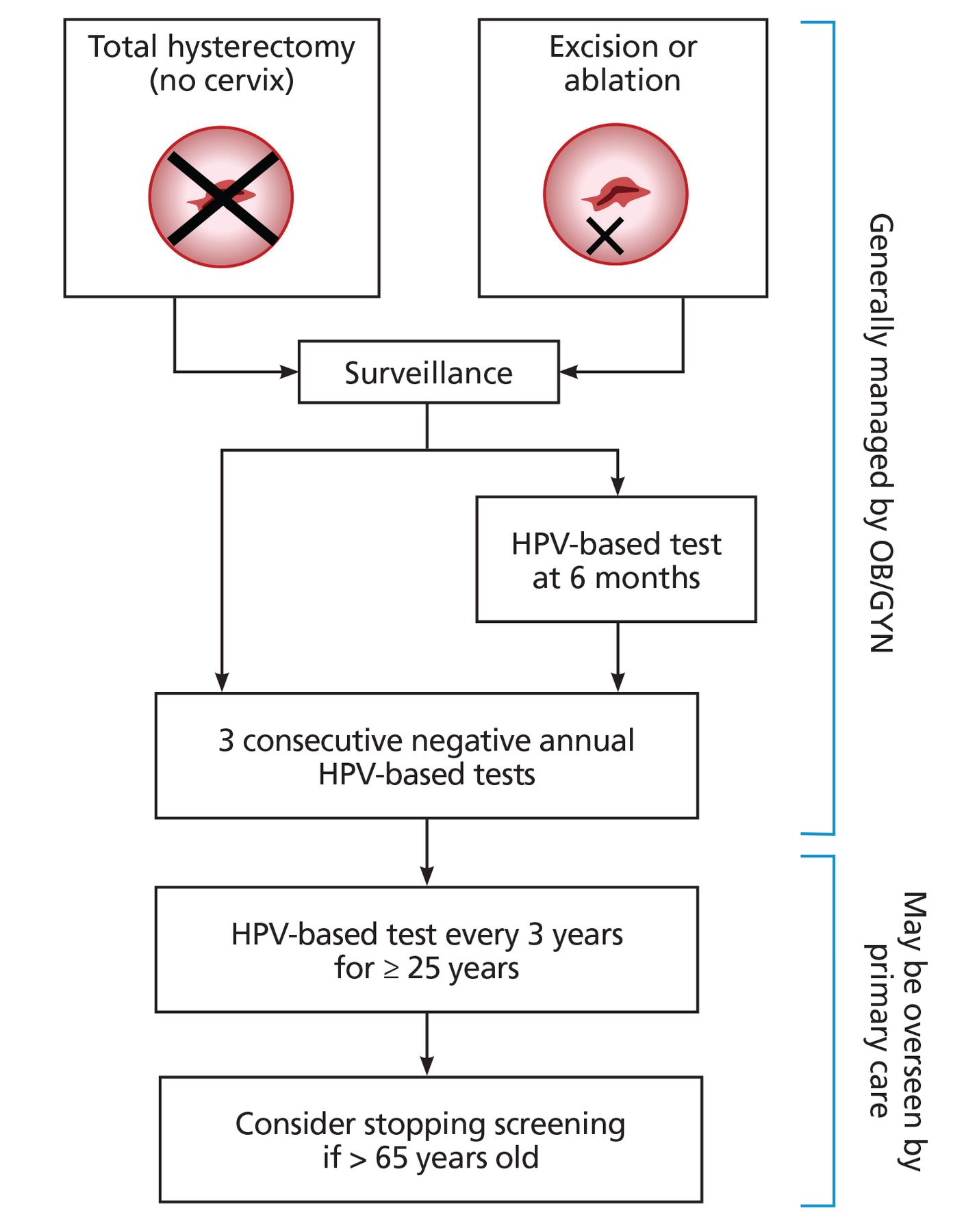
Management and surveillance for patients with a history of high-grade cervical dysplasia (high-grade squamous intraepithelial lesion, cervical intraepithelial 2 or 3, or adenocarcinoma in situ).
HPV = human papillomavirus; OB/GYN = Obstetrics and Gynecology


Tables
Organization Recommended screening test and frequency 2018 US Preventive Services Task Force13 Age < 21 years
No screeningAge 21–29 years
Cervical cytology (Pap test) every 3 yearsAge 30–65 years
Choose betweenCervical cytology (Pap test) every 3 years, or
Primary HPV testing every 5 years, or
Cotesting every 5 years
2020 American Cancer Society12 Age 25–65 years
Primary HPV testing every 5 years preferredAcceptable alternatives (given access to primary HPV testing may be limited): Cotesting every 5 years, or
Cervical cytology (Pap test) every 3 years
HPV = human papillomavirus; Pap = Papanicolaou
Age > 65 years, if… After hysterectomy, if… Patient is asymptomatic, and Total hysterectomy (removal of the cervix) was performed,a and Has no history of CIN2 or worse in the past 25 years, and Hysterectomy was performed for benign indication, and Has undergone adequate prior screening: 3 consecutive negative cytology results in past 10 years with most recent within 3 years, or
2 consecutive negative HPV test results in past 10 years with most recent within 5 years
There is no history of high-grade precancerous lesion (eg, CIN2 or worse) in the past 25 years or history of HPV-related lower genital tract cancer ↵a Patients who have undergone a hysterectomy and retained the cervix (subtotal or supracervical hysterectomy) should continue screening per guidelines for average- or high-risk screening, as clinically appropriate.
CIN2 = cervical intraepithelial grade 2; HPV = human papillomavirus
Based on information in references 12 and 13.
Calcineurin inhibitors Cytotoxic agents mTOR inhibitors Steroids Biologics Monoclonal antibodies Tacrolimus (Crohn; non-FDA)
Cyclosporine (UC; non-FDA)Mycophenolate
Azathioprine (IBD; non-FDA)
Leflunomide (Crohn; non-FDA)
Chlorambucil
Cyclophosphamide
Mercaptopurine (IBD; non-FDA)
Methotrexate (Crohn; non-FDA)
Platinum compounds
Fluorouracil
DactinomycinSirolimus
EverolimusPrednisone (IBD; FDA)
Prednisolone (IBD; FDA)
Budesonide (IBD; FDA)
Dexamethasone (IBD; FDA)Abatacept
Adalimumab (IBD; FDA)
Anakinra
Apremilast
Certolizumab (Crohn; FDA)
Etanercept (Crohn; non-FDA)
Golimumab (UC; FDA)
Infliximab (IBD; FDA)
Ixekizumab
Natalizumab (Crohn; FDA; (UC; non-FDA)
Rituximab
Secukinumab
Tocilizumab
Ustekinumab (Crohn; FDA)
Vedolizumab (IBD; FDA)Basiliximab
Daclizumab
MuromonabFDA = US Food and Drug Administration; IBD = inflammatory bowel disease; mTOR = mammalian target of rapamycin; UC = ulcerative colitis
Reprinted from Moscicki AB, et al. Guidelines for cervical cancer screening in immunosuppressed women without HIV infection. J Low Genit Tract Dis 2019; 23(2):87–101. doi:10.1097/LGT.0000000000000468 with permission from Wolters Kluwer Health.
Screening Age to start Age to stop Recommended test and frequency Rationale Screening should begin at time of diagnosis but not before age 21 Screening should continue throughout a patient’s lifetime (considering life expectancy)a Age < 30 years
Cytology (Pap test) at baseline, then annually
If 3 consecutive Pap tests are normal, then cytology every 3 years (until age 30)Age ≥ 30 years
Choose between cytology (Pap test) at baseline, then annually (if not already completed before age 30); if 3 consecutive Pap tests are normal, then cytology every 3 years or cotesting every 3 yearsBegin screening at age 21 to provide a 3–5-year window before age 25, when the risk of invasive cervical cancer in patients with HIV exceeds that of the general population20; while historically screening was done before age 21, patients rarely develop cervical cancer before age 2121
In patients age < 30, cotesting is not recommended due to a high prevalence of transient HPV in this age group3Management Regardless of age, colposcopy is recommended in the following scenarios: HPV-positive ASC-US; if HPV testing is not performed, then repeat cytology in 6–12 months is recommended, with colposcopy referral for ASC-US or worse
All cytology results of low-grade squamous intraepithelial lesion or worse (including ASC-H, atypical glandular cells, adenocarcinoma in situ, and high-grade squamous intraepithelial lesion) regardless of HPV test results (if completed)
↵a If a patient with HIV undergoes a hysterectomy with removal of cervix (total hysterectomy) for benign disease and has no history of cervical intraepithelial neoplasia 2+, then ongoing routine screening for cervical or vaginal cancer is generally not recommended.
ASC-H = atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion; ASC-US = atypical squamous cells of undetermined significance; HIV = human immunodeficiency virus; HPV = human papillomavirus; Pap = Papanicolaou
Data from references 3 and 16.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.