


ABSTRACT
The recommended duration of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention with a drug-eluting stent has changed from 1 year for all to a more personalized approach based on the patient’s risks of ischemia and bleeding. The trend is toward shorter treatment in view of lower rates of late and very late stent thrombosis with newer drug-eluting stents and the risk of bleeding with DAPT. But some patients at high risk of ischemic events and low risk of bleeding may benefit from longer treatment.
A shorter duration of DAPT (< 12 months) is favored for patients at high risk of bleeding or low risk of ischemia, or both.
DAPT for 12 months or more should be considered for patients at high risk of ischemic events (eg, due to prior myocardial infarction) and at low risk of bleeding.
For patients on DAPT who need noncardiac surgery, 3 factors should be considered: risk of bleeding if surgery is performed while the patient continues DAPT; risk of stent thrombosis if DAPT is interrupted; and consequences of delaying surgery. For some, a bridging protocol can be used.
Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor after a percutaneous intervention (PCI) is one of the most commonly prescribed therapies in cardiovascular medicine. However, treatment strategies have evolved as our understanding of stent thrombosis has deepened and stents have improved, leading to uncertainty, even among cardiologists, about how to best manage DAPT.
This article reviews current guidelines on the duration of therapy and perioperative management of DAPT after PCI (Table 1).
Dual antiplatelet therapy (DAPT) after percutaneous coronary intervention with a drug-eluting stent
BEYOND THE RIGID 1-YEAR RECOMMENDATION
Bare-metal stents, developed to keep an artery open after angioplasty, were associated with stent thrombosis and restenosis, requiring repeat revascularization in many patients.1 The risk of stent thrombosis was found to be mitigated by aspirin and 1 month of ticlopidine, sparking the initial enthusiasm for DAPT as we know it today.2
Drug-eluting stents were subsequently developed to reduce the risk of stent restenosis.1 However, concerns about late and very late stent thrombosis with first-generation drug-eluting stents precipitated the need for longer DAPT. Trials at the time assessed 1 year of therapy, and when it was found to be effective, it became the reference duration of DAPT after drug-eluting stent placement, regardless of the clinical presentation at the time of PCI.3,4
Second-generation drug-eluting stents have better polymers and smaller struts and are associated with significantly lower rates of late and very late stent thrombosis.1 These improvements propelled the use of drug-eluting stents rather than bare-metal stents, and they became the predominantly placed stent, even in patients for whom the duration of DAPT must be shorter.5 However, increased bleeding with prolonged DAPT remained a major drawback, so an extensive evaluation of DAPT duration was undertaken. Knowing how long and under what conditions to continue DAPT after drug-eluting stent PCI is critical for best managing these patients.
Shorter DAPT for some patients
The 2016 American College of Cardiology and American Heart Association (ACC/AHA)6 guidelines and the 2017 European Society of Cardiology (ESC)7 guidelines provide the most recent updates on DAPT management. Despite subtle differences, their overall message is the same. The rigid recommendation for 1 year of DAPT after PCI with a drug-eluting stent irrespective of indication has been revised, and a new paradigm has been introduced. DAPT duration is now determined by balancing risk of future ischemic events against bleeding (Figure 1).
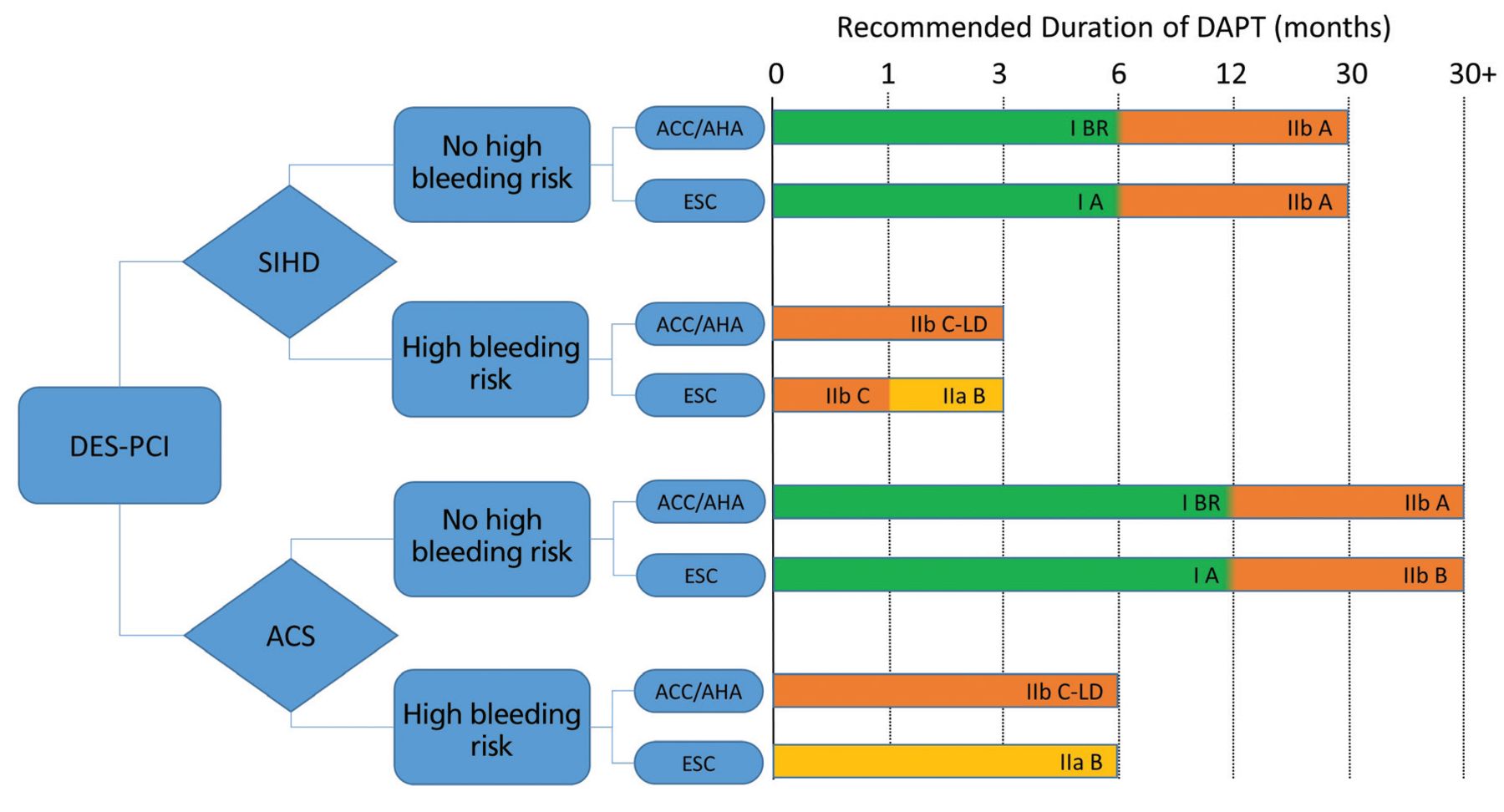
Recommended duration of dual antiplatelet therapy after percutaneous coronary intervention with drug-eluting stents. Class of recommendation and level of evidence: class I, benefit much greater than risk; class II, benefit greater than risk, with conflicting evidence or opinion; class IIa, weight of evidence or opinion is in favor of usefulness; class IIb, usefulness is less well established. Level of evidence: A, from multiple randomized clinical trials; B or BR, from one or more randomized trials; C or C-LD, from nonrandomized observational studies.
ACC = American College of Cardiology; ACS = acute coronary syndrome; AHA = American Heart Association; DAPT = dual antiplatelet therapy; DES = drug-eluting stent; ESC = European Society of Cardiology; PCI = percutaneous coronary intervention; SIHD = stable ischemic heart disease
For patients with an acute coronary syndrome treated with a drug-eluting stent, at least 12 months of DAPT is recommended. However, just 6 months can be considered for those with high bleeding risk.
For patients with stable ischemic heart disease treated with a drug-eluting stent, at least 6 months of DAPT with clopidogrel is recommended, but just 3 months can be considered for those at high bleeding risk, or even just 1 month if 3 months of DAPT poses safety concerns.
These guidelines were based on multiple randomized controlled trials over the previous decade that compared 6 months or less of DAPT with longer durations after PCI with a drug-eluting stent.8–14 Meta-analyses of these trials demonstrated that in an all-comers population, regardless of PCI indication and underlying comorbidities, shorter durations of DAPT decrease bleeding at the expense of increased ischemic events, eg, stent thrombosis and myocardial infarction.15–17 Further exploration of the data behind this conclusion illuminates the intricacies of DAPT management and provides the foundation for the current guidelines.
BALANCING RISKS
Bleeding risk from DAPT is directly proportional to the length of therapy, with longer periods leading to increased bleeding events and higher rates of noncardiovascular mortality.15 On the other hand, the reduction of ischemic events from DAPT is greatest in the first few weeks due to protection from early stent thrombosis. Over time, the benefit from protection against stent thrombosis decreases, and the predominant advantage of DAPT shifts to protection from spontaneous myocardial infarction, ie, from plaque rupture at sites remote from the stented index lesion.18
Despite the reduction of stent thrombosis and myocardial infarction with persistent DAPT, cardiac mortality rates are the same with 6 months or less of therapy compared with longer durations.15 This is likely due to the declining mortality risk of stent thrombosis over time and the inclusion of smaller myocardial infarctions with less prognostic relevance in trial end points.19 Consequently, there is no effect on all-cause mortality comparing 6 months or less vs 1 year of DAPT.15 Thus, it can be reasoned that patients at high risk of bleeding, low risk of ischemic events, or both, may benefit from a shorter duration of DAPT, and those at low risk of bleeding, high risk of ischemic events, or both, may benefit from a longer duration.
Although no study has exclusively focused on patients with stable ischemic heart disease who received drug-eluting stents, subgroup analyses demonstrate that they are at much lower risk of stent thrombosis and myocardial infarction,20 hence the adequacy of DAPT for 6 months according to the most recent guidelines. The recommendations for patients with an acute coronary syndrome and high bleeding risk are based on the same logic. They were supported in the 2018 SMART-DATE trial (Safety of 6-month Duration of Dual Antiplatelet Therapy After Acute Coronary Syndrome),21 which demonstrated a higher risk of myocardial infarction in patients with acute coronary syndrome who received DAPT for 6 months compared with 12 or more months. But no difference was found in all-cause mortality with longer DAPT due to the higher incidence of bleeding.
INTERRUPT DAPT FOR NONCARDIAC SURGERY?
When patients on DAPT after drug-eluting stent PCI need noncardiac surgery, one must consider:
The risk of bleeding from surgery if DAPT is continued
The risk of stent thrombosis if DAPT is interrupted
The consequences of delaying surgery.
These are complicated questions but can be approached in a disciplined manner.
The risk of bleeding during surgery is higher for a patient on antiplatelet therapy.22,23 Given the increased mortality and morbidity associated with bleeding,24 antiplatelet therapy should be minimized before surgery unless it can be performed with minimal bleeding risk while on DAPT. However, because DAPT significantly reduces the risk of stent thrombosis, and interruption of DAPT after stent placement is one of the strongest risk factors for stent thrombosis,6 the tension between the risks of bleeding and stent thrombosis must be balanced. When possible, this dilemma can be solved by delaying surgery. However, in many situations (eg, for malignant and vascular diseases), delaying surgery can be detrimental.25,26
Multiple observational studies have tried to determine a time frame after stenting when the risk of DAPT interruption is low enough for patients to undergo surgery.27–29 Older observational studies based on bare-metal stents and mostly first-generation drug-eluting stents found that the risk of stent-related thrombotic complications is highest in the first 4 to 6 weeks but continues to be elevated for at least 1 year.27 More recent observational studies suggest the time frame of increased risk is about 6 months,28 and may even be as short as 30 days.29
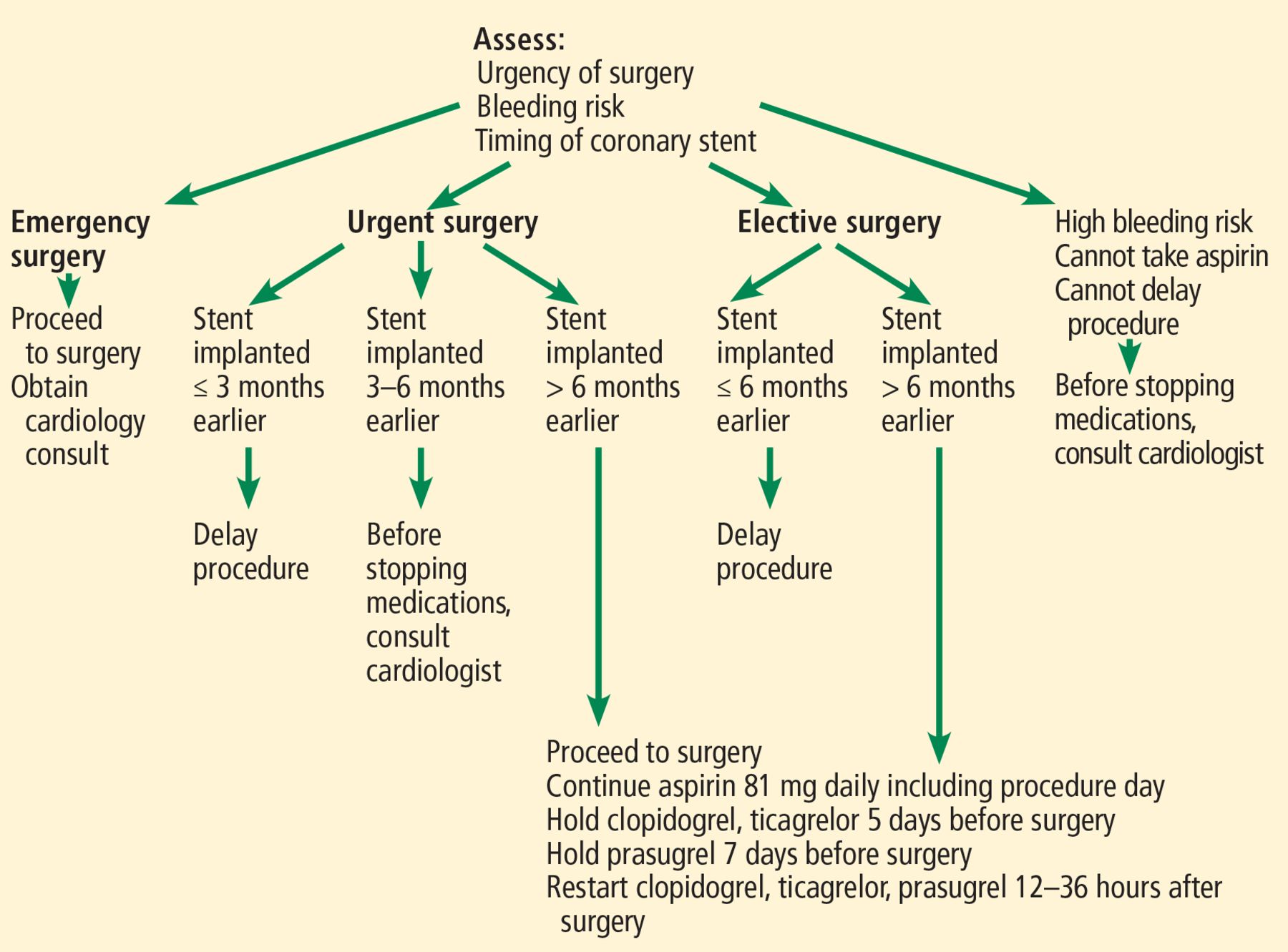
Based on these data, Cleveland Clinic uses the approach shown in Figure 2. Developed by a multidisciplinary team of specialists, the algorithm balances the risks of bleeding, stent thrombosis, and delaying surgery and is similar to the one in the ACC/AHA guidelines.6
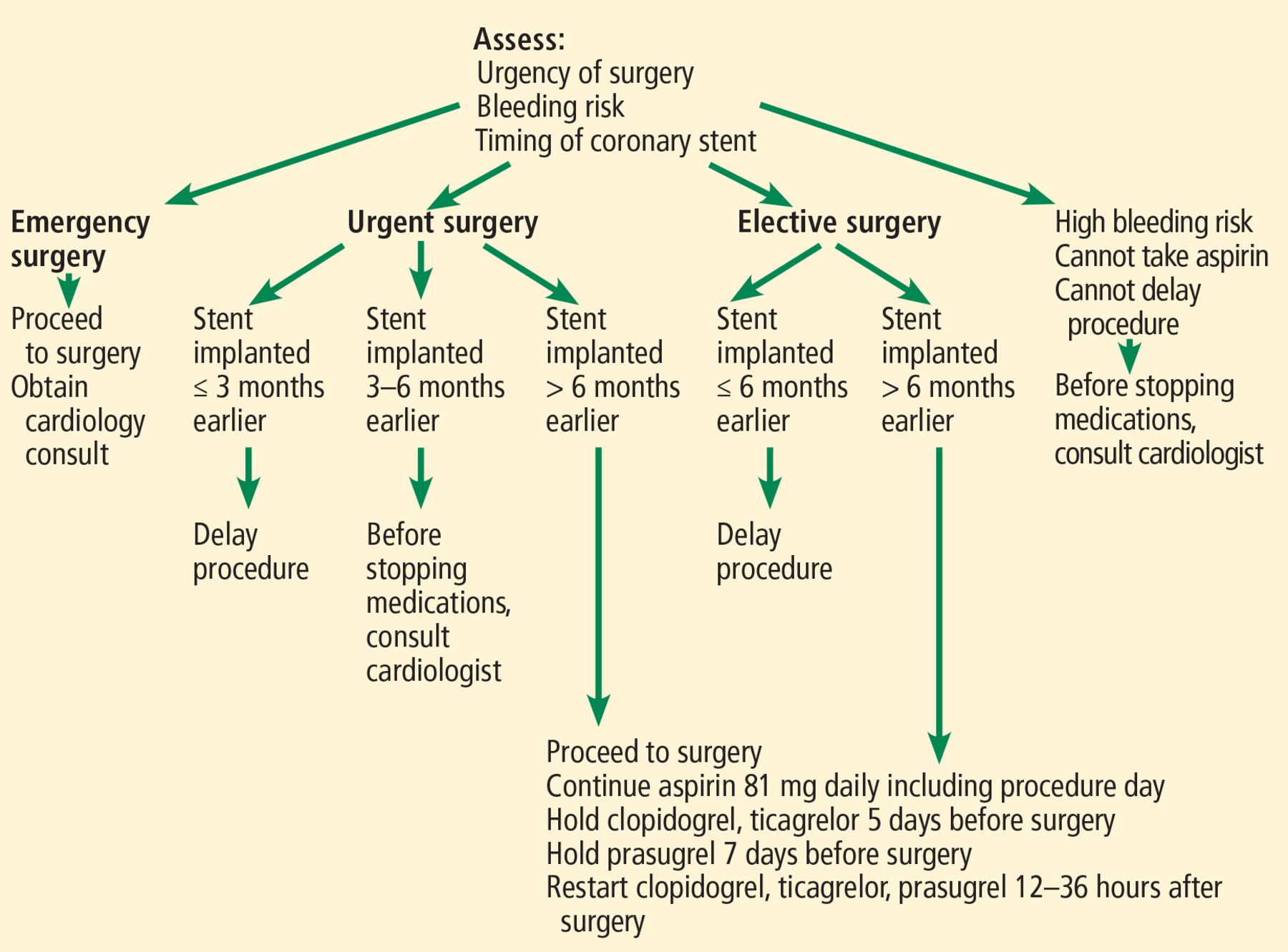
Guidelines for preoperative management of patients with coronary stents undergoing noncardiac surgery.
If DAPT is interrupted, aspirin should be continued if feasible, as it protects against ischemic events,30 and P2Y12 therapy should be restarted as soon as possible.6,7 If the risk of stent thrombosis is particularly high and surgery cannot be delayed, it should be performed in hospitals where heart catheterization is readily available, and bridging with intravenous antiplatelet agents should be considered.6,7 Our approach to intravenous antiplatelet bridging is shown in Figure 3.

Guidelines for bridging before surgery in patients with prior coronary stent.
WHO NEEDS LONGER DAPT?
Whether DAPT is beneficial for longer than 12 months has been debated for many years. After the first-generation drug-eluting stents were introduced and 12 months was subsequently identified as the standard DAPT duration, multiple trials have investigated whether extending DAPT further would be useful.8,11,17,31–33 As for determining whether shorter DAPT duration could be indicated, risk of future ischemic events was balanced against bleeding.
The first and largest study to investigate this question18 found that in patients who completed 12 months of DAPT after PCI without suffering an ischemic or bleeding event, continuing DAPT for 18 additional months reduced myocardial infarction and stent thrombosis rates but increased major bleeding and mortality compared with patients taking aspirin and placebo. The increase in mortality was driven by noncardiovascular causes. Subgroup analysis found that in patients with a prior myocardial infarction, the reduction in ischemic events was most pronounced and survival was greatest, although overall mortality was still neutral in this population. Subsequent meta-analyses of this and other randomized controlled trials comparing more than 12 months of DAPT and shorter durations demonstrated similar findings.34,35 Notably, some of these trials enrolled patients with first- and second-generation drug-eluting stents, and a subgroup analysis of the DAPT trial showed significant attenuation of benefit in those with second-generation drug-eluting stents.36
Attention subsequently turned to prolonged DAPT in patients with a prior myocardial infarction. The PEGASUS TIMI 54 trial (Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared With Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54) tested prolonged DAPT in patients who had a myocardial infarction in the previous 1 to 3 years.33 It found a reduction in most ischemic end points but no effect on the rate of all-cause mortality. These results were confirmed in a meta-analysis of the PEGASUS trial plus subgroups from 4 additional randomized controlled trials.37
Based on these findings, clinical decision-making surrounding more than 12 months of DAPT therapy requires an individualized appraisal of the risk and benefits. As discussed previously, with safer, newer-generation drug-eluting stents, the largest benefit of long-term DAPT is reduction of spontaneous myocardial infarction. This highlights the shift from local stent-related protection of early DAPT to systemic protection with longer therapy.
Bottom line. Long-term DAPT should only be considered in patients with a prior myocardial infarction who are at high risk of recurrence and low risk of bleeding (class of recommendation IIb).6,7 The PRECISE-DAPT score and the DAPT score can be used to help determine if a patient may benefit from prolonged therapy.7
The PRECISE-DAPT score (www.pre-cisedaptscore.com) is based on the patient’s:
Hemoglobin level
White blood cell count
Age
Creatinine clearance rate
History of bleeding.
The DAPT score (http://tools.acc.org/daptriskapp/#!/content/calculator/) is based on the following:
Age
Cigarette smoking
Diabetes mellitus
Myocardial infarction
Prior PCI or prior myocardial infarction
Paclitaxel-eluting stent
Stent diameter less than 3 mm
Congestive heart failure or left ventricular ejection fraction less than 30%
Placement of a stent in a vein graft.
In patients who discontinue P2Y12 inhibitors, current recommendations are to continue aspirin indefinitely for cardiac protection. However, as noted below, this is an area of active research to identify the best option to ensure protection from cardiovascular risk while reducing the risk of bleeding.
FUTURE DIRECTIONS
In the future, DAPT management will likely continue to focus on defining the optimal level of platelet inhibition at various stages of post-PCI and tailoring therapy appropriately. Since much of the data underpinning current guidelines on DAPT management was accrued from observational studies with first-and second-generation drug-eluting stents, future guidelines will likely accept even shorter durations of DAPT for most patients, and provide considerations for P2Y12 monotherapy.
The recently published TWILIGHT (Ticagrelor With or Without Aspirin in High-Risk Patients After Coronary Intervention) trial emphasizes this model.38 Patients at high risk of bleeding and ischemic events who completed 3 months of DAPT were randomized to continue DAPT or receive ticagrelor monotherapy for 12 months. Bleeding rates were significantly lower in the monotherapy group without a statistically significant increase in ischemic events. A 2020 meta-analysis of multiple similar trials confirmed these findings.39
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.