


ABSTRACT
Bulimia nervosa, a mental illness 4 times more common than anorexia nervosa, is characterized by binge-eating followed by compensatory purging behaviors, which include self-induced vomiting, diuretic abuse, laxative abuse, and misuse of insulin. Patients with bulimia nervosa are at risk of developing medical complications that affect all body systems, especially the renal and electrolyte systems. Behavior cessation can reverse some, but not all, medical complications.
Most people with bulimia nervosa are young and of normal weight, or even overweight, making detection and diagnosis difficult.
As a consequence of purging behaviors, pseudo-Bartter syndrome can develop due to chronic dehydration, placing patients at risk for electrolyte abnormalities such as hypokalemia, as well as marked and rapid edema formation when purging is interrupted.
Electrolyte and metabolic disturbances are the most common causes of morbidity and mortality in patients with bulimia nervosa. Hypokalemia should be managed aggressively to prevent electrocardiographic changes and arrhythmias such as torsades de pointes.
Diabetic patients who purge calories through manipulation of their blood glucose are at high risk for hyperglycemia, ketoacidosis, and premature microvascular complications.
Gastrointestinal complaints are common and include gastroesophageal reflux disease.
A 21-year-old woman with a history of depression and anxiety presents to your clinic for follow-up after an emergency room visit, where she had presented 2 days earlier for feeling like she was going “to pass out” during her college cross-country meet. At the emergency room, the patient was noted to have a serum potassium level of 2.9 mmol/L (reference range 3.7–5.1 mmol/L), bicarbonate 35 mmol/L (22–30 mmol/L), and orthostatic hypotension. She was given 2 L of intravenous normal saline and intravenous and oral potassium.
On follow-up, her vital signs are normal. Her body mass index is 24.5 kg/m2. She reports feeling better but has noted marked swelling of both her lower extremities, which is causing her distress. The examination is notable for bilateral 2+ pitting edema and calluses on the dorsal aspect of her right hand.
A SERIOUS MENTAL ILLNESS WITH PHYSICAL CONSEQUENCES
Bulimia nervosa (BN) is a serious mental illness characterized by binge-eating followed by compensatory purging behaviors. It is frequently accompanied by medical sequelae that affect normal physiologic functioning and contribute to increased morbidity and mortality rates.1 Most people with BN are of normal weight or even overweight,2 and are otherwise often able to avoid detection of their eating disorder. Thus, it is important that clinicians familiarize themselves with these complications and how to identify patients with disordered eating patterns.
Recurrent binge-eating followed by purging
BN is characterized by overvaluation of body weight and shape and recurrent binge-eating (consuming an excessive caloric amount in a short period of time, usually a 2-hour period, that the patient feels unable to control). This is soon accompanied by compensatory purging behaviors that can include abuse of laxatives and diuretics, withholding insulin (termed diabulimia or eating disorder-diabetes mellitus type 1), self-induced vomiting, fasting, and excessive exercise. Some patients also abuse caffeine or prescription stimulant medications commonly used to treat attention-deficit/hyperactivity disorder.
Self-induced vomiting and laxative misuse account for more than 90% of purging behaviors in BN.3 The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) requires episodes of bingeing and compensatory behaviors in BN to occur at least once per week over the course of 3 months and not occur during an episode of anorexia nervosa.3 The complications of purging behaviors found in BN are identical to those found in the binge-purge subtype of anorexia nervosa except that restriction of calories primarily and excessive weight loss are not present.
The severity of BN is determined by the frequency of the mode of the purging behaviors (mild: an average of 1–3 episodes of inappropriate compensatory behaviors weekly; moderate: 4–7; severe: 8–13; extreme: 14 or more) or the degree of functional impairment.2 Some patients may vomit multiple times per day while others may use significant amounts of laxatives. Some may engage in multiple different purging behaviors, which has been shown to be associated with a greater severity of illness.4 Exercise is considered excessive if it interferes with other activities, persists despite injury or medical complications, or occurs at inappropriate times or situations.2,5
ONSET IN ADOLESCENCE, AND FAIRLY COMMON
BN typically develops in adolescence or young adulthood and affects both sexes, although it is much more common in girls and young women.6 It affects people regardless of sexual orientation but has been shown to be more prevalent in nonheterosexual males.7 Studies have found similar prevalence of BN among different racial and ethnic groups. Individuals with BN are generally within or above the normal weight range.2
According to pooled data from the World Health Organization, the lifetime prevalence of BN in adults is 1.0% using the older DSM-IV criteria,7 which is greater than the reported prevalence of anorexia nervosa. Prevalence estimates are higher with the broadened DSM-5 criteria, ranging from 4% to 6.7%.8
There are multiple predisposing and perpetuating factors—genetic, environmental, psychosocial, neurobiological, and temperamental. These can include impulsivity, developmental transitions such as puberty, internalization of the thin ideal, and weight and shape concerns.9 A history of childhood trauma, including sexual, physical or emotional trauma, has also been associated with BN.10
More than 70% of people with eating disorders report concomitant psychiatric comorbidity—affective disorders, anxiety, substance use, and personality disorders are most common in BN.11 Psychiatric comorbidities as well as hopelessness, shame, and impulsivity associated with the illness may contribute to challenges with nonsuicidal self-harm, suicidal ideation, and death by suicide. Individuals with BN experience lifetime rates of nonsuicidal self-harm of 33% and are nearly 8 times more likely to die by suicide than the general population.12,13 The reported standardized mortality rates in those with BN are less than in those with anorexia nervosa but are still significantly elevated at 1.5% to 2.5%.1
MEDICAL COMPLICATIONS
As noted earlier, BN is associated with a significantly increased mortality rate even though many of these patients are young. Much of this elevated mortality is attributable to the medical complications associated with BN, which are a direct result of the mode and frequency of purging behaviors. Thus, for example, if someone uses laxatives 3 times per day or vomits 1 time per day, there may be no medical complications, but many patients engage in their respective purging behaviors many times per day, leading to multiple complications.
Aside from the electrolyte aberrations from purging, some of the medical complications are unique to the mode of purging. Furthermore, BN has been found to increase the risk of any cardiovascular disease, including ischemic heart disease and death in females.14 These same complications may also apply to patients with anorexia nervosa of the binge-purge subtype in contrast to those patients with anorexia nervosa who only restrict caloric intake but do not purge.
We will now discuss, in a systems-based approach, the medical complications that develop in people with BN as a direct result of their purging behaviors.
Skin
Russell sign (Figure 1), named after Dr. Gerald Russell, who first defined the disease BN in 1979, refers to the development of calluses on the dorsal aspect of the dominant hand.15 It is pathognomonic for self-induced vomiting and is due to traumatic irritation of the hand by the teeth, from repeated insertion of the hand into the mouth to provoke vomiting.15

The Russell sign.
Russell sign is not commonly seen since many of these patients are able to spontaneously vomit or they utilize utensils to initiate self-induced vomiting.
Teeth and mouth
Abnormalities of the teeth and mouth, specific for purging via vomiting, include dental erosions and trauma to the oral mucosa and pharynx.16
Dental erosion is the most common oral manifestation of chronic regurgitation. It is believed to be caused by the teeth coming into contact with acidic vomitus (pH 3.8), although just how changes in salivary composition and dietary intake contribute is unclear. It tends to affect the lingual surfaces of the maxillary teeth and is known as perimyolysis. Vomiting also potentially increases the risk of dental caries.
Trauma to the oral mucosa, especially the pharynx and soft palate, is also encountered and is presumed to occur either as a result of the patient inserting a foreign object into the mouth to induce vomiting or the caustic effect of the vomitus on the mucosal lining.
Dental erosions are irreversible once they have developed. Use of fluorinated mouth wash after purging and horizontal gentle brushing are recommended. Ongoing self-induced vomiting will also damage newly implanted teeth as well as dental prosthetics.
Head, ears, nose, and throat
Purging by vomiting increases the risk of sub-conjunctival hemorrhages from forceful retching, which can also cause recurrent epistaxis. Indeed, recurrent bouts of epistaxis that remain unexplained should prompt a search for covert BN.
Pharyngitis is often noted in those who vomit frequently, due to contact of the pharyngeal tissue with stomach acid. Hoarseness, cough, and dysphagia may also similarly develop. Pharyngeal and laryngeal complaints can be improved with cessation of vomiting and the use of medications to suppress acid production, such as proton pump inhibitors.
Parotid glands
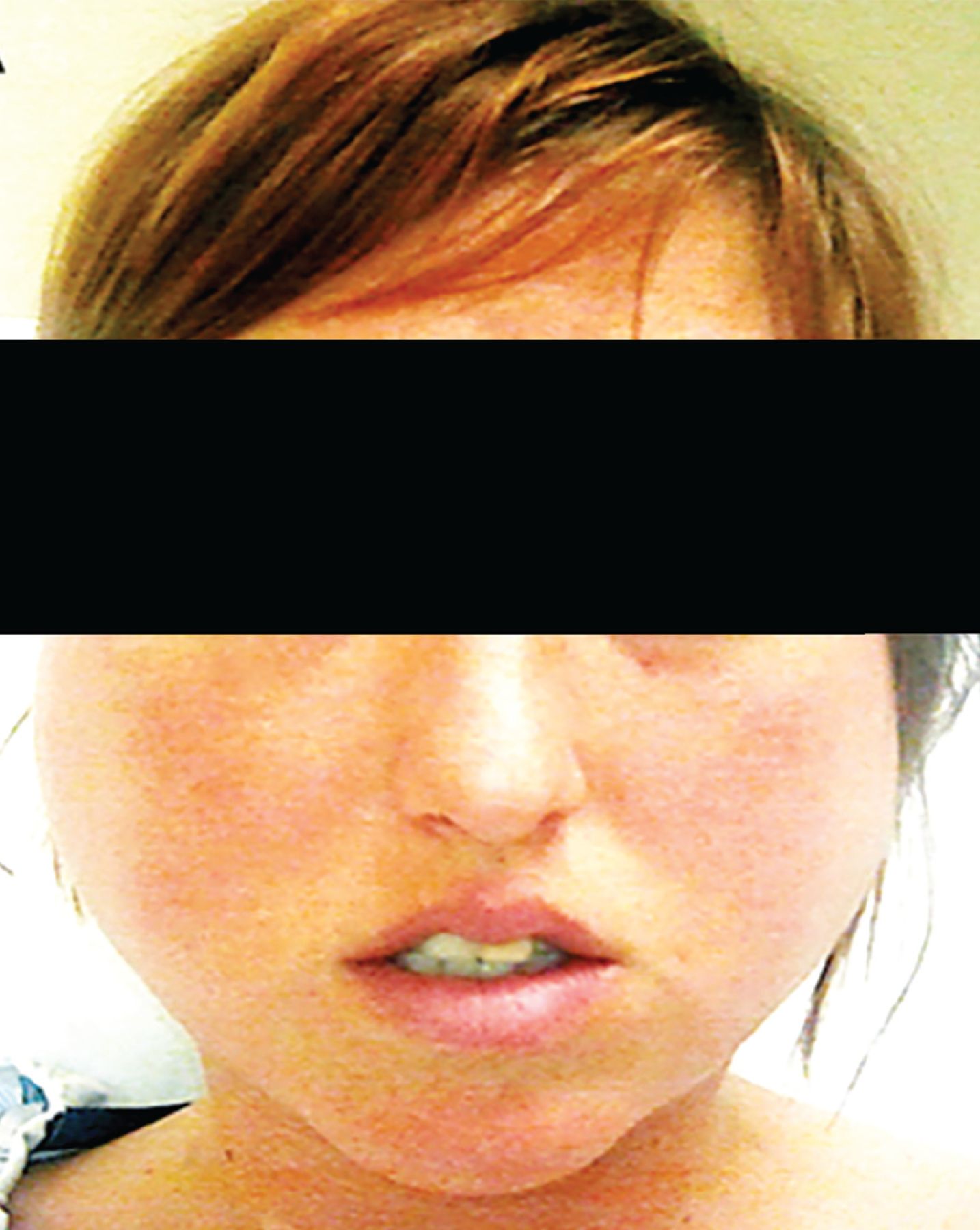
Parotid gland hypertrophy, or sialadenosis (Figure 2), may develop in more than 50% of people engaging in purging via self-induced vomiting.17 Ironically, it usually develops 3 to 4 days after cessation of purging. Symptoms include bilateral painless enlargement of the parotid glands and, occasionally, other salivary glands. It is believed to develop due to either cholinergic stimulation of the glands, hypertrophy of the glands to help meet demands of increased saliva production, or excessive backup of saliva that is no longer needed with cessation of vomiting.
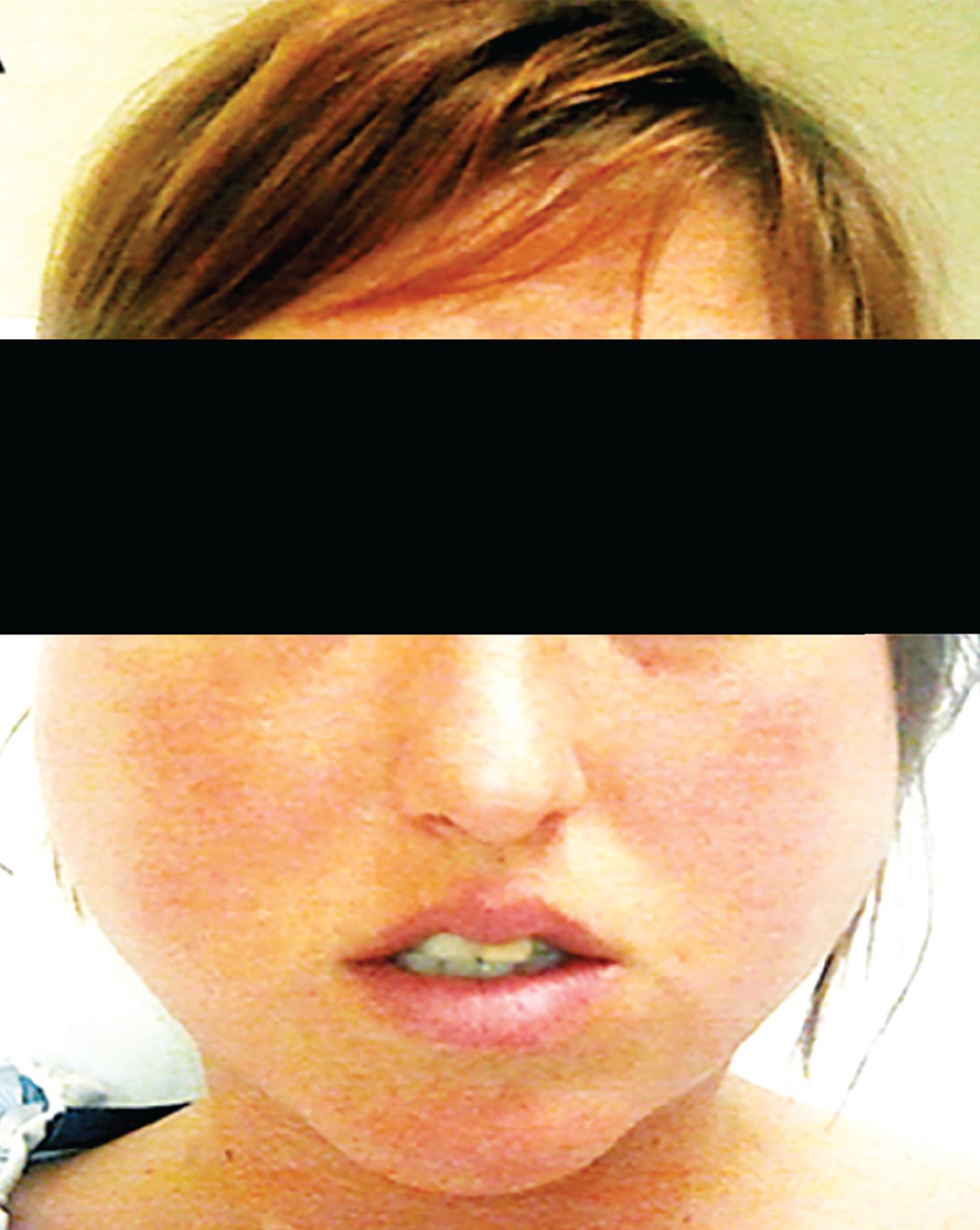
Sialadenosis.
Pathology study reveals hypertrophied acinar cells with otherwise preserved architecture without evidence of inflammation.
Swelling may subside with cessation of purging; failure of the parotid gland hypertrophy to resolve is highly suggestive of ongoing purging.18 Sialadenosis also tends to resolve with the use of sialagogues such as tart candies. Heating pads and nonsteroidal anti-inflammatory drugs also have a therapeutic role and perhaps should be prophylactically initiated in those with a long history of excessive vomiting who engage in treatment to stop purging. In rare refractory cases, pilocarpine may be judiciously used to reduce the glands back to normal size.19
Cardiovascular
The cardiac complications that are specific for purging include electrolyte disturbances as a result of vomiting and diuretic or laxative abuse. Conduction disturbances, including serious arrhythmias and QT prolongation, are increasingly encountered in those participating in various modes of purging due to the electrolyte disturbances that ensue, especially hypokalemia and acid-base disorders. Also, excessive ingestion of ipecac, which contains the cardiotoxic alkaloid emetine, to induce vomiting can lead to various conduction disturbances and potentially irreversible cardiomyopathy.20
Abuse of caffeine or stimulant medications used to treat attention-deficit/hyperactivity disorder may cause palpitations, sinus tachycardia, or cardiac arrhythmias such as supra-ventricular tachycardia. Similarly, diet pill abuse, which is increased in this population, is associated with arrhythmias.21
Pulmonary
Retching during vomiting increases intrathoracic and intra-alveolar pressures, which can lead to pneumomediastinum.22 Pneumomediastinum may also be encountered due to nontraumatic alveolar rupture in the setting of malnutrition and is therefore nonspecific in differentiating patients who purge from those who restrict.23 Vomiting also increases the risk of aspiration pneumonia. Aspiration may be involved in the heretofore enigmatic pathogenesis of pulmonary infection with Mycobacterium avium complex organisms.
Gastrointestinal
The gastrointestinal complications of purging depend on the mode of purging used. Upper gastrointestinal complications develop in those who engage in vomiting, whereas lower gastrointestinal complications develop in those who abuse stimulant laxatives.
Esophageal complications. Excessive vomiting exposes the esophagus to gastric acid and damages the lower esophageal sphincter, increasing the propensity for gastroesophageal reflux disease and other esophageal complications, including Barrett esophagus and esophageal adenocarcinoma.24 However, it is unclear if there truly is an association between purging by self-induced vomiting and reflux disease. Although research indicates increased complaints of gastrointestinal reflux disease in those engaging in purging, and increased reflux may be present in those who purge when assessed by pH monitoring, endoscopic findings do not necessarily correlate with severity of reported symptoms.24,25 This suggests a possible functional component to gastrointestinal reflux-related concerns.26
Cessation of purging is the recommended treatment, although proton pump inhibitors can be tried. Metoclopramide may also be beneficial, given its actions of accelerating gastric emptying and increasing lower esophageal sphincter tone. Endoscopy should be considered if symptoms continue or have been present for many years, to look for the precancerous esophageal mucosal abnormalities found in Barrett esophagus.
Rare complications are esophageal rupture, known as Boerhaave syndrome, and Mallory-Weiss tears, causing upper gastrointestinal bleeds due to the recurrent episodes of emesis. Mallory-Weiss tears commonly present as blood-streaked or tinged emesis or scant coffee ground emesis following recurrent vomiting episodes. Usually blood loss from such tears is minimal. Mallory-Weiss tears appear as longitudinal mucosal lacerations on endoscopy.
Colonic inertia. Individuals engaging in excessive and chronic stimulant laxative abuse may be at risk for “cathartic colon,” a condition whereby the colon becomes an inert tube incapable of moving stool forward. This is believed due to direct damage to the gut myenteric nerve plexus.27 However, it is currently speculative as to whether this condition truly develops in those with eating disorders and with use of currently available stimulant laxatives.28 Regardless, in general, stimulant laxatives should be used only short-term, due to concerns regarding potential development of this condition, and should be stopped in those in whom it develops. Instead, osmotic laxatives, which do not directly stimulate peristalsis, are prescribed in a measured manner to manage constipation.
Melanosis coli, a black discoloration of the colon of no known clinical significance, is often reported during colonoscopy in those abusing stimulant laxatives. Rectal prolapse may also develop in those abusing stimulant laxatives, but again is nonspecific for this mode of purging as it can also develop solely as a consequence of malnutrition and the resultant weakness of the pelvic floor muscles.
Endocrine
A potential endocrine complication of BN is irregular menses,29 as opposed to the amenorrhea frequently observed in both the restricting and binge-purge subtypes of anorexia nervosa.
Although patients with BN do not appear to be at a significantly increased risk for low bone mineral density—in contrast to those suffering from the restricting and binge-purge subtypes of anorexia nervosa—a bone density scan with dual-energy x-ray absorptiometry may still be warranted to evaluate for bone disease in those with a past history of anorexia nervosa.
Patients with type 1 diabetes mellitus may manipulate their blood glucose levels as a means to purge calories, a condition previously referred to as diabulimia and now termed eating disorder-diabetes mellitus type 1.30 These patients are at risk of marked hyperglycemia, ketoacidosis, and premature microvascular complications such as retinopathy and neuropathy.
METABOLIC AND ELECTROLYTE DISTURBANCES
In addition to the above body system complications from purging, each of the common methods of purging used by patients with BN can be associated with specific electrolyte disturbances. These electrolyte abnormalities are likely the most proximate cause of death in patients with BN. When a patient simultaneously engages in multiple modes of purging behaviors, just as their level of psychiatric illness can be more profound, so too the electrolyte disturbance profiles can overlap and be more extreme.
Patients with a history of a known purging behavior should be screened at increased frequency for serum electrolyte disturbances, up to even daily, depending on the frequency of their purging behaviors.31 In a study of patients admitted to inpatient and residential eating disorder treatment without prior medical stabilization, 26.2% of the BN patients presented with hypokalemia (potassium < 3.6 mmol/L) on their admission laboratory testing, while 8.5% had hyponatremia (sodium < 135 mmol/L) and 23.4% had a metabolic alkalosis (bicarbonate > 28 mmol/L).32
Self-induced vomiting is the most common method of purging in BN.33 Patients with self-induced vomiting or diuretic abuse, or both, have been shown to present with hypokalemia, hypochloremia, and a metabolic alkalosis.34 The severity of the electrolyte abnormalities worsens with the frequency of vomiting.
Similarly, laxative abuse also results in hypokalemia and hypochloremia. However, either a non-anion gap metabolic acidosis or a metabolic alkalosis may be present, depending on the chronicity of the laxative abuse.35 Generally, more chronic diarrhea results in a metabolic alkalosis. Hyponatremia can also be present with these 3 purging behaviors. The hyponatremia encountered is most often of the hypovolemic type due to chronic fluid depletion as a result of the purging behaviors.
Pathophysiology of hypokalemia and hypochloremia
The pathophysiologic reasons for hypokalemia and hypochloremia seen with all significant purging behaviors are 2-fold and interrelated. First, and most obvious, there is loss of potassium in the purged gastric contents, excessive stool from laxative abuse, or in the urine through diuretic abuse.
Second, chronic purging results in intravascular fluid depletion. This fluid depletion is sensed by the afferent arteriole of the kidney as decreased renal perfusion pressure, which in turn activates the renin-angiotensin-aldosterone system, resulting in increased production of aldosterone by the zona glomerulosa of the adrenal glands. Aldosterone acts renally at the distal convoluted tubules and cortical collecting ducts, causing them to resorb sodium and chloride in the body’s attempt to prevent severe dehydration, hypotension, and fainting. Aldosterone also promotes renal secretion of potassium into the urine and thus hypokalemia. This mechanism of potassium loss is actually a larger contributor to the hypokalemia than the actual gastrointestinal or urinary loses from the behaviors themselves.
The mechanisms by which metabolic alkalosis occurs in self-induced vomiting and in laxative abuse are similar. Initially, hydrogen ions and sodium chloride are lost in the vomitus or through diarrhea. The loss of hydrogen ions produces an alkalemic state. Intravascular volume depletion resulting from the loss of sodium chloride increases the resorption of bicarbonate within the proximal renal tubule, preventing its loss in the urine, which would normally occur to correct the alkalemia. Hypokalemia, if concurrently present, also increases bicarbonate resorption in the proximal tubule, further propagating the metabolic alkalosis. Lastly, increased serum aldosterone levels, brought about from intravascular volume depletion, fuel resorption of sodium at the expense of hydrogen and potassium, resulting in increased loss of hydrogen and potassium in the urine and further maintenance of the alkalemic state.
In diuretic abuse, the diuretics themselves act directly on the kidney to promote loss of sodium chloride in the urine, resulting in intravascular depletion and aldosterone secretion. This results in loss of hydrogen and potassium into the urine, resulting in a metabolic alkalosis. Potassium-sparing diuretics, such as spironolactone, however, do not precipitate a metabolic alkalosis, as they inhibit the action of aldosterone in the kidney.
Table 1 summarizes the electrolyte derangements that occur with BN.
Summary of electrolyte disturbances in bulimia nervosa
PSEUDO-BARTTER SYNDROME
The aforementioned process of renin-angiotensin-aldosterone system activation results in what has been termed pseudo-Bartter syndrome due to resulting serum and histochemical findings on renal biopsy that resemble Bartter syndrome.36 However, the findings are not due to intrinsic renal pathology but rather are a result of the chronic state of dehydration from the purging behaviors. The resultant elevation in serum aldosterone, an integral part of pseudo-Bartter syndrome, can result in rapid edema formation when the purging behaviors are abruptly stopped. The reason is that the serum aldosterone levels remain high, causing salt and water retention even though the patient is no longer losing fluid, as the purging has ceased.
EVALUATION AND MANAGEMENT OF ELECTROLYTE DISTURBANCES AND PSEUDO-BARTTER SYNDROME
Covert purging should be strongly suspected in otherwise healthy young women presenting with hypokalemia without an alternative medical cause.37 However, hypokalemia alone is not specific for underlying purging behaviors.34
If the patient is not forthcoming about their behavior when confronted, a spot urine potassium, creatinine, sodium, and chloride measurement can be obtained to further assess the source of potassium loss. A urine potassium-to-creatinine ratio less than 13 can identify hypokalemia resulting from gastrointestinal loss, diuretics, poor intake, or transcellular shifts. A urine sodium-to-chloride ratio can also be calculated. Vomiting is associated with a urine sodium-to-chloride ratio greater than 1.6 in the setting of hypokalemia, whereas laxative abuse is associated with a ratio less than 0.7.36
Chronic hypokalemia is often asymptomatic and can be corrected slowly. If the serum potassium level is no lower than 2.5 mmol/L and the patient has no physical symptoms or electrocardiographic changes of hypokalemia, the hypokalemia can be managed by stopping the purging behavior and giving oral potassium supplementation.38,39 Adherence to oral potassium repletion can be improved by using potassium chloride tablets rather than liquid preparations.38 Aggressive intravenous potassium supplementation places patients at risk of hyperkalemia and should be reserved for more critically low serum potassium levels.
Severe hypokalemia (serum potassium less than 2.5 mmol/L) requires both oral and intravenous repletion of potassium. This repletion process is aided by giving isotonic saline with potassium chloride intravenously at a low infusion rate (50–75 mL/hour). Correcting the patient’s volume depletion is required to correct the metabolic alkalosis and interrupt renin-angiotensin-aldosterone system activation. Untreated severe hypokalemia can result in a prolonged corrected QT interval on electrocardiography, subsequent torsades de pointes, and other life-threatening cardiac arrhythmias. Simply attempting to replete potassium without attention to the concomitant metabolic alkalosis will be unsuccessful because of the ongoing kaliuresis due to aldosterone’s ongoing effects on the kidneys. Rarely, chronic hypokalemia has been associated with acute renal failure, with renal biopsy demonstrating interstitial nephritis, termed hypokalemic nephropathy.40
Mild hyponatremia often will autocorrect with interruption of purging behaviors and oral rehydration. However, if the serum sodium is less than 125 mmol/L, hospitalization is warranted for close monitoring and for slow correction with isotonic saline—ie, at a rate that increases the serum sodium by no more than 4 to 6 mmol/L every 24 hours. This avoids the serious complication known as central pontine myelinolysis.41 If hyponatremia is severe (serum sodium < 118 mmol/L), the patient will likely benefit from admission to an intensive care unit and renal consultation for consideration of administration of desmopressin to prevent overcorrection.
Metabolic alkalosis can develop in patients with BN as a result of decreased intravascular volume, elevated aldosterone, and hypokalemia; it is most often saline-responsive. A spot urine chloride can be used to inform care. If it is less than 10 mmol/L, the metabolic alkalosis is hypovolemic and will improve with slow intravenous saline administration. Clinicians may also rely on physical examination to help determine the patient’s volume status.
Due to the underlying risk of pseudo-Bartter syndrome in patients with BN who abruptly stop purging, care should be taken to avoid aggressive fluid resuscitation. Interruption of purging behaviors in conjunction with rapid intravenous fluid resuscitation can result in marked and rapid edema formation and weight gain, which can be psychologically distressing. Thus, low infusion rates of saline (50 mL/hour) and low doses of spironolactone (50–100 mg initially with a maximum of 200–400 mg/day) should be initiated and titrated based on edema and weight trends to mitigate edema formation.42 Spironolactone is generally continued for 2 to 4 weeks and then should be tapered by 50 mg every few days thereafter. Occasionally, in extreme laxative abusers, proclivity toward edema may persist and necessitate an even slower spironolactone taper.
MEDICAL COMPLICATIONS OF BINGE-EATING
The literature on complications of binge-eating specific to BN is limited, and thus, we must look to studies of binge-eating disorder. However, patients with binge-eating disorder tend to be overweight or obese, as they do not purge after binge episodes. Thus, many of the medical complications in binge-eating disorder, such as type 2 diabetes, hypertension, nonalcoholic fatty liver disease, and metabolic syndrome are obesity-related.43
In contrast, many patients with BN have a normal body mass index. Therefore, it is difficult to infer that the medical complications that occur in binge-eating disorder are the same as those that occur from binge-eating in BN. However, the extrapolation does make sense in some instances. For instance, patients who binge are at higher risk of nutritional deficiencies because food taken in during a binge tends to be processed, high in fat and carbohydrates, and low in protein. A diet low in vitamins, including A and C, and minerals increases the risk of nutritional deficiencies. Additionally, patients with binge-eating disorder have more gastrointestinal complaints such as acid reflux, dysphagia, and bloating, which, as outlined above, are also seen in BN. Thus, bingeing may play a role in these symptoms.
Lastly, gastric perforation has been reported in patients with BN in the context of a bingeing episode marked by excessive stomach distention, resulting in gastric necrosis.44 Furthermore, gastric outlet obstruction has also been reported in this patient population due to formation of a food bezoar.
IDENTIFICATION AND MENTAL HEALTH TREATMENT
The Eating Disorder Screen for Primary Care has been shown to effectively screen patients for disordered eating in a general medicine setting.45 It consists of 5 questions:
Are you satisfied with your eating pattern? (“No” is considered an abnormal response.)
Do you ever eat in secret? (“Yes” is an abnormal response to this and the remaining questions.)
Does your weight affect the way you feel about yourself?
Have any members of your family suffered from an eating disorder?
Do you currently suffer with or have you ever suffered in the past with an eating disorder?
Cotton et al45 found that an abnormal response to 2 or more of these questions had a sensitivity of 100% and a specificity of 71% for eating disorders.
Standard mental health treatments for BN include nutritional stabilization and behavior interruption, monitoring for and appropriate management of associated medical complications, prescribing medications as clinically indicated, and psychotherapeutic interventions. Cognitive behavioral therapy is the recommended initial intervention for the treatment of BN. A recent network meta-analysis suggested that guided cognitive behavioral self-help and a specific form of cognitive behavioral therapy—individual cognitive behavioral therapy for eating disorders—may most likely lead to full remission.46
No drug has been developed specifically for the treatment of BN (Table 2). Fluoxetine, with a target dose of 60 mg daily independent of the presence of comorbidities, is the only medication approved by the US Food and Drug Administration for BN. This selective serotonin reuptake inhibitor has been shown to reduce the frequency of binge-eating and purging episodes significantly, more so than fluoxetine 20 mg daily and placebo.47 Fluoxetine is recommended for patients who do not respond adequately to psychotherapeutic interventions.48
Psychopharmacology clinical pearls
Other selective serotonin reuptake inhibitor antidepressants along with the anti-epileptic topiramate also have been shown to have modest efficacy.49 Bupropion, which has a boxed warning and is contraindicated in the treatment of BN, should not be used due to an increased risk of seizure.
No clinical trials have evaluated the use of stimulant medications in the treatment of BN. Often, stimulant medications are discontinued in patients until there is a period of abstinence from purging behaviors. Following abstinence, reinitiation of the stimulant could be reconsidered off-label if bingeing behaviors persist or attention deficit hyperactivity disorder is a comorbidity, or both. There can be some utility to reinitiation with a clear treatment agreement outlining expectations for maintaining efforts at purging symptom interruption and continued stimulant prescribing.
In general, concomitant treatment for anxiety or depression should be pursued if these co-occur with BN. Selective serotonin reuptake inhibitors such as fluoxetine would also target these symptoms. If a trial of fluoxetine has failed, then sertraline or escitalopram would be reasonable second-line options. Typically, citalopram would not be used due to higher risk of prolonged QT interval than other selective serotonin reuptake inhibitors, especially given the possibility of electrolyte abnormalities in BN. Paroxetine would not be used due to the potential for weight gain as a side effect.
PROGNOSIS
Increased risk of relapse has been associated with greater psychosocial dysfunction and body image disturbance.50 In patients requiring hospitalization, a number of factors have been shown to predict poor outcome, including fewer follow-up years, increased drive for thinness, older age at initial treatment, and more impairment in global functioning.50 Recovery is possible with variable remission rates, based on the type of study and definition of remission, from 38% and 42% at 11-and 21-year follow-up, respectively, and 65% of individuals at a 9-year and 22-year follow-up.50,51 This reinforces the need to utilize accessible and effective treatments to achieve sustained recovery.
CONCLUSION
BN is a complex psychiatric disease with myriad medical complications, some of which may be life-threatening. Most of the morbidity and mortality in patients with BN is a direct result of the aforementioned purging behaviors and their resultant electrolyte and acid-base disorders. Thus, it is important that clinicians familiarize themselves with these complications as most patients with BN are of normal weight and are otherwise often able to avoid detection of their eating disorder.
INITIAL CASE CONTINUED
You release the patient in the initial clinical scenario from her follow-up appointment without intervention or follow-up laboratory testing. You fail to recognize the Russell sign, and you advise her that the edema is due to fluids administered in the emergency department and will self-resolve. She returns to her purging behaviors with increased vigor due to perceived weight gain from the edema.
One month later, she experiences a syncopal episode during cross-country practice, again necessitating oral potassium and intravenous saline administration. On follow-up, her edema is worse, and you recognize the Russell sign, having just read this review article. On follow-up laboratory testing, you note ongoing mild hypokalemia and screen her for an eating disorder. The screening is positive, and she discloses to you not only about her daily self-induced vomiting, but also her abuse of stimulant laxatives and bingeing episodes.
You initiate a referral to a residential treatment facility for eating disorders, start her on daily potassium chloride 40 mmol, and plan for weekly follow-up laboratory testing until she enters residential treatment.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgments
The authors would like to thank Ms. Kelly Maebane for her superb assistance with formatting and editing of the manuscript.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- A SERIOUS MENTAL ILLNESS WITH PHYSICAL CONSEQUENCES
- ONSET IN ADOLESCENCE, AND FAIRLY COMMON
- MEDICAL COMPLICATIONS
- METABOLIC AND ELECTROLYTE DISTURBANCES
- PSEUDO-BARTTER SYNDROME
- EVALUATION AND MANAGEMENT OF ELECTROLYTE DISTURBANCES AND PSEUDO-BARTTER SYNDROME
- MEDICAL COMPLICATIONS OF BINGE-EATING
- IDENTIFICATION AND MENTAL HEALTH TREATMENT
- PROGNOSIS
- CONCLUSION
- INITIAL CASE CONTINUED
- DISCLOSURES
- Acknowledgments
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.