


Article Figures & Data
Figures
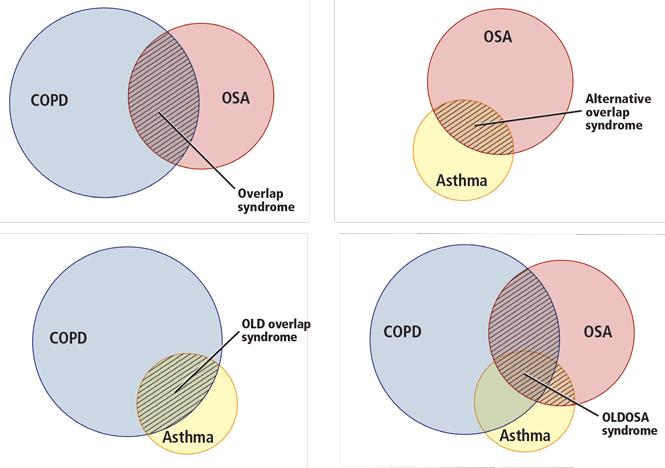
- FIGURE 2
The main overlap syndromes. Sizes of circles roughly correspond to prevalences of the diseases they represent. COPD = chronic obstructive pulmonary disease; OLD = obstructive lung disease; OLDOSA = obstructive lung disease and obstructive sleep apnea; OSA = obstructive sleep apnea. OLD overlap syndrome has also been called asthma-COPD overlap syndrome.
Based on Ioachimescu OC, Teodorescu M. Integrating the overlap of obstructive lung disease and obstructive sleep apnoea: OLDOSA syndrome. Respirology 2013; 18:421–431; with permission from John Wiley & Sons, Inc.

Tables
Feature Asthma COPD Exceptions and overlapping features Risk factors Allergens Smoking Smoking may be an aggravating factor in asthma; children with early-life wheezing have a higher risk of developing asthma as teenagers and chronic obstructive pulmonary disease (COPD) as adults (the “Dutch hypothesis”); repeated airway infections may trigger development of either asthma or COPD, depending on the nature of infection and the intrinsic genetic predisposition (the “British hypothesis”) Anatomic segment involved Airways Airways and parenchyma Severe asthma exacerbations may lead to adjacent parenchymal destruction, severe hyperinflation, and loss of scaffolding, or to radial or axial traction, or both, on the small airways Atopy Yes No Atopy may be present in some patients with COPD Airway inflammation Yes Yes Absent in mild asthma between exacerbations Peripheral eosinophilia Yes No Some patients with COPD may have eosinophilia; some patients with asthma may have neutrophilic infiltration (eg, severe asthma, asthma coexistent with gastroesophageal reflux and chronic rhinitis) Airway eosinophilia Yes No 20%–40% of patients with COPD have airway eosinophilia (if one excludes eosinophilic bronchitis, up to 20% patients with COPD can still have some eosinophilic airway infiltration) Exhaled gas (lower-airway) nitric oxide concentration High Low May be reduced in some asthma phenotypes, eg, neutrophilic or paucigranulocytic; may be present in some patients with COPD Diffusing lung capacity for carbon monoxide Normal Reduced (in emphysema) Normal in chronic bronchitis; increased in acute asthma Airway resistance High High Normal in mild asthma between exacerbations; normal or slightly increased in emphysema Airway hyperresponsiveness Yes No May be present in COPD Elastic recoil of the airways and parenchyma Normal Reduced (in emphysema) Reduced in acute exacerbations of severe asthma; normal in chronic bronchitis Symptoms Episodic Persistent May be episodic in some patients with COPD, especially during significant environmental exposures Comorbidities Atopic dermatitis, allergic rhinitis Cardiovascular disease Obstructive sleep apnea may complicate both conditions - TABLE 2
Proposed ABCD-3P-PQRST characterization system for asthma phenotypes, genotypes, and endotypes
ABCD 3P modela PQRST Asthmaticsymptoms Paroxysmal (< 1 month)
Persistent (1–6 months)
Permanent (> 6 months)Precipitating factors Exertion (during, after), allergens, odors, drugs, tobacco smoke Qualitative description Cough, wheezing, chest tightness, dyspnea Reversibility to bronchodilator Absolute change, percent change Severity Mild intermittent, mild, moderate, severe, or very severe persistent Type Onset (adulthood or childhood), race and ethnicity, gender (male or female, prepubertal, adult, postmenopausal) Biomarkers Predominant cells Effector cells: eosinophils, neutrophils, mast cells, mixed cellularity, paucicellular
Lymphocytes: T-helper 1 (Th1), Th2, Th17, regulatory T lymphocyes, natural killer cellsPredominant cytokines, immunoglobulins, molecules Interleukin (IL) 4, IL-5, IL-9, IL-13, IL-33, periostin; interferon gamma, IL-15, IL-17, IL-18, IL-21, IL-22; immunoglobulin E or G; nitric oxide Predisposing genotype Specific gene polymorphisms, mutations Conditions associated Prenatal risk factors Maternal smoking, diet, nutrition, antibiotic use, stress Postnatal risk factors Early-life wheezing, breastfeeding, early tobacco smoke exposure, viral infections, vitamin D deficiency, contact with animals, occupational exposures Pathogenically linked conditions Atopy, allergic rhinitis, chronic rhinosinusitis, nasal polyposis, obstructive sleep apnea, gastroesophageal reflux disease, obesity, bronchiectases Drugs used Anticholinergics (short-acting and long-acting), beta-2 adrenergic agonists (short-acting and long-acting), corticosteroids (inhaled, oral), leukotriene pathway-modifying agents (eg, leukotriene receptor agonists, lipooxygenase inhibitors), phosphodiesterase inhibitors (eg, theophylline, rofl umilast), cromolyn, nedocromil, mast cell stabilizers, anti–IL-5 agents (eg, mepolizumab, benralizumab, reslizumab), anti–IL-13 agents (eg, lebrikizumab, tralokinumab), anti-IgE (eg, omalizumab), anti-tumor necrosis factor alpha (golimumab) ↵a 3P model for disease persistence should be characterized clinically, functionally, and biologically (eg, including exhaled gas concentration of nitric oxide).




{kind=link}
{kind=link}