


Article Figures & Data
Figures
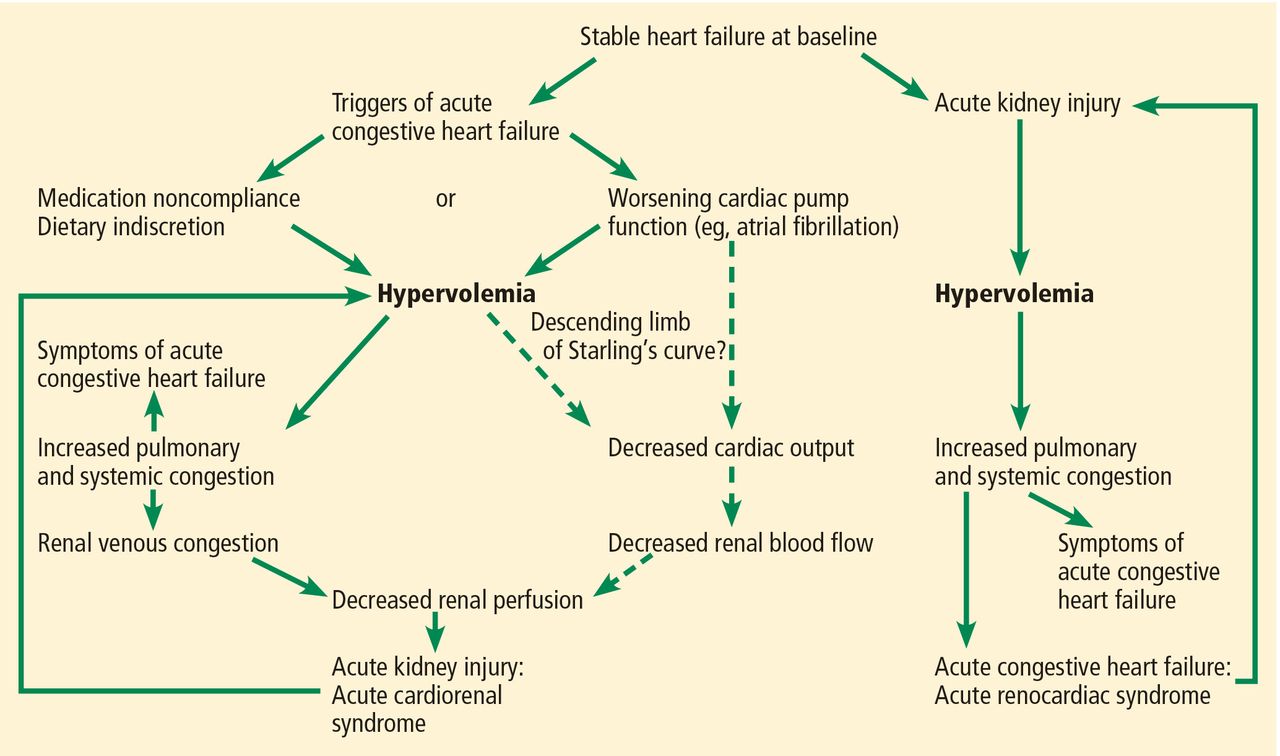
- FIGURE 1
Hemodynamic derangements in acute cardiorenal and renocardiac syndromes. Hypervolemia plays a central role. Dashed arrows indicate noncritical pathways.
Tables
General definition
Disorders of the heart and kidneys in which acute or chronic dysfunction in one organ may induce acute or chronic dysfunction of the otherType 1: Acute cardiorenal syndrome
Acute worsening of cardiac function leading to renal dysfunctionType 2: Chronic cardiorenal syndrome
Chronic abnormalities in cardiac function leading to renal dysfunctionType 3: Acute renocardiac syndrome
Acute worsening of renal function causing cardiac dysfunctionType 4: Chronic renocardiac syndrome
Chronic abnormalities in renal function leading to cardiac diseaseType 5: Secondary cardiorenal syndromes
Systemic conditions causing simultaneous dysfunction of the heart and kidneyFrom House AA, Anand I, Bellomo R, et al. Definition and classification of cardio-renal syndromes: workgroup statements from the 7th ADQI Consensus Conference. Nephrol Dial Transplant 2010; 25:1416–1420.
Loop diuretics: maximum intravenous bolus dose Drug Creatinine clearance < 25 mL/min Creatinine clearance 25–75 mL/min Creatinine clearance > 75 mL/min Furosemide 160–200 mga 80–160 mga 40–80 mga Bumetanide 8–10 mga 4–8 mga 1–2 mga Torsemide 50–100 mga 20–50 mga 10–20 mga Loop diuretics: continuous infusion Drug Creatinine clearance < 25 mL/min Creatinine clearance 25–75 mL/min Creatinine clearance > 75 mL/min Furosemide 40-mg loading dose, then 20 mg/hour × 1 hour; if response is inadequate, repeat loading dose and increase infusion to 40 mg/hour 40-mg loading dose, then 10 mg/hour × 1 hour; if response is inadequate, repeat loading dose and increase infusion to 20 mg/hour 40-mg loading dose, then 10 mg/hour × 1 hour; if response is inadequate, repeat loading dose and increase infusion to 20 mg/hour Bumetanide 1-mg loading dose, then 1 mg/hour × 1 hour; if response is inadequate, increase infusion to 2 mg/hour 1-mg loading dose, then 0.5 mg/hour × 1 hour; if response is inadequate, repeat loading dose and increase infusion to 1 mg/hour 1-mg loading dose, then 0.5 mg/hour Torsemide 20-mg loading dose, then 10 mg/hour × 1 hour; if response is inadequate, increase infusion to 20 mg/hour 20-mg loading dose, then 5 mg/hour × 1 hour; if response is inadequate, increase infusion to 10 mg/hour 20-mg loading dose, then 5 mg/hour Thiazide diuretics Drug Creatinine clearance < 20 mL/min Creatinine clearance 20–50 mL/min Creatinine clearance > 50 mL/min Hydrochlorothiazide 100–200 mg/day 50–100 mg/day 25–50 mg/day Chlorothiazide Usual dosage range: 500–2,000 mg/day in 1 or 2 divided dosesb Metolazone Usual dosage range: 2.5–20 mg once dailyb Carbonic anhydrase inhibitor Acetazolamide Usual dosage range: 250–1,000 mg/day in 1 or 2 divided doses




{kind=link}
{kind=link}