


ABSTRACT
Recent trials evaluated the impact of aspirin for primary prevention of cardiovascular events in patients at intermediate risk, patients with diabetes, and the elderly, and the results have been incorporated into the most recent professional guidelines. For the most part, the role of aspirin in primary prevention remains limited, albeit not adequately tested in those at higher risk.
Using aspirin for the sole purpose of primary prevention is discouraged in healthy elderly patients (age > 70) and those at high risk of bleeding, including patients on anticoagulation.
Routine use of aspirin for the sole purpose of primary prevention is best deferred in patients at low risk (< 5% 10-year risk) and borderline risk (5%-7.5% 10-year risk). However, in selected patients at borderline risk, such as those with a strong family history, clinicians could also consider risk-enhancers such as coronary calcium.
A shared decision to initiate aspirin in those at intermediate risk (7.5%-20% 10-year risk) could be considered for patients with a risk-enhancer such as an elevated coronary calcium score (> 100) or elevated lipoprotein(a) (> 50 mg/dL).
In patients age 40 to 70 at high risk (> 20% at 10 years), it is reasonable to consider starting low-dose aspirin as a shared decision if the patient is thought to be at low risk of bleeding.
Aspirin is one of the most widely used drugs in cardiovascular medicine, with one-third of adults over the age of 40 using it for either primary or secondary prevention of major cardiovascular events. But does this widespread use achieve the intended goal of reducing the incidence of cardiovascular events and death?
The use of aspirin undoubtedly reduces the risk of a subsequent cardiovascular event or death from vascular causes when used for secondary prevention—eg, in patients who have had a myocardial infarction, stroke, or symptomatic peripheral arterial disease or who have undergone coronary revascularization.1-5 However, its net impact in primary prevention (ie, in patients without established cardiovascular disease or previous coronary revascularization) has been debated for years.5-7
Recent clinical trials have reevaluated the role of aspirin in primary prevention.8-12 The results suggest that aspirin should play a more limited role than in the past, and this evidence has resulted in an update in the recommendations from the American Heart Association (AHA) and American College of Cardiology (ACC).13
This review examines the evidence on the risk-benefit profile of aspirin in primary prevention of cardiovascular events (Table 1),8-12,14-24 summarizes current recommendations on this topic, and proposes an evidence-based algorithm to guide the use of aspirin for primary prevention in clinical practice.
Trials of aspirin as primary prevention
CONFLICTING EVIDENCE FROM OLDER TRIALS
ATC meta-analysis, 2009
The Anti-thrombotic Trialists’ Collaboration (ATC) meta-analysis, published in 2009, was a landmark study of the role of aspirin in primary prevention.5 It analyzed patient-level data from 6 trials published between 1988 and 2005,14-19 mostly addressing the impact of aspirin in patients at low risk, with an event rate of about 0.5% per year (or 5% in 10 years).
Serious vascular events (myocardial infarction, stroke, and vascular death) occurred at a rate of 0.51% per year in the aspirin groups and 0.57% in the placebo groups. Although this represented a 12% reduction in relative risk (relative risk [RR] 0.88, 95% confidence interval [CI] 0.82-0.94, P = .0001), the absolute risk reduction was very modest: 1,667 patients would need to be treated for 1 year (or 167 for 10 years) to prevent 1 major cardiovascular event. This reduction was primarily driven by a reduction in nonfatal myocardial infarctions and ischemic strokes but not in vascular mortality.
Although all the prespecified subgroups showed a similar proportional reduction in major cardiovascular events, the data suggested that men and women might benefit differently from aspirin. Men primarily experienced a reduction in nonfatal myocardial infarctions, while women benefited from a reduction in ischemic strokes.5,20 However, this differential effect was not noted in the secondary prevention cohort of the meta-analysis and was no longer statistically significant when accounting for multiple comparisons.
The modest reduction in nonfatal cardiovascular events came at the cost of excess bleeding—and 1 in every 4 events was a hemorrhagic stroke. Major extracranial bleeding occurred in 0.10% of the aspirin recipients and 0.07% of the placebo recipients, and hemorrhagic stroke occurred in 0.04% vs 0.03%, for an increase of 0.04% per year in the rate of major bleeding. Thus, 1 major bleeding event would be caused after treating 333 patients for 10 years. Based on this evidence, 2 nonfatal cardiovascular events would be prevented per major bleed caused.
Hence, the net impact of aspirin for primary prevention of major cardiovascular events was at best marginal in these earlier trials, mainly reducing the incidence of nonfatal cardiovascular events and largely counterbalanced by the risk of bleeding.
Also, at the time these data were gathered, best preventive practices and aspirin dosing significantly differed from the current standard of care. Today, tighter blood pressure control, lower rates of smoking, and widespread use of statins likely make the risk-benefit profile of aspirin in primary prevention less favorable. For instance, using a statin halves the benefit of aspirin without attenuating the bleeding risk, which could completely dissipate the marginal benefit reported in the ATC metaanalysis and perhaps render aspirin harmful in patients at low risk.5
Despite the very modest benefits reported in these early trials, debate continued as to whether the net impact would be more favorable in patients at higher risk of cardiovascular events. Evidence supporting this notion was that the relative risk reduction in major cardiovascular events was about the same in both primary prevention (RR 0.88, 95% CI 0.82-0.94) and secondary prevention (RR 0.81, 95% CI 0.82-1.00).5 For context, giving aspirin in the secondary prevention cohort resulted in a 1.5%-per-year absolute reduction (number needed to treat 7 for 10 years) in the annual rate of major cardiovascular events compared with the marginal absolute reduction of 0.07% per year (number needed to treat 167 for 10 years) in the primary prevention cohort. This difference in absolute benefit is due to the substantially higher baseline rate of cardiovascular events in the secondary prevention group.
Further studies, 2008-2014
Hence, a second wave of studies, published between 2008 and 2014, sought to evaluate the impact of aspirin for primary prevention in a higher-risk population, ie, patients with diabetes, low ankle-brachial index, or other cardiovascular risk factors.21-24 Despite this intention, these trials, like the earlier ones, largely studied a low-risk population. Only in the Prevention of Progression of Arterial Disease and Diabetes trial was the event risk greater than 1% per year (or > 10% in 10 years).21
Most of these studies were small and therefore lacked the power to detect differences in cardiovascular event rates, with only the Japanese Primary Prevention Project having a sample size comparable to the earlier trials.22
Collectively, these studies failed to show any benefit of aspirin for primary prevention of major cardiovascular events, and even the better-powered Japanese Primary Prevention Project was stopped early due to futility regarding the composite end point of death, myocardial infarction, and stroke. Although an overall negative trial, this was the only study from 2008 to 2014 to report a potential reduction in nonfatal myocardial infarction as a secondary end point, a suggested benefit that was largely counterbalanced by a higher rate of major bleeding.22
The negative results of these studies came as a surprise and greatly contrasted with the at-least marginal benefit reported by the earlier trials. These results were attributed in part to lack of statistical power but also to improved management of cardiovascular risk factors with tighter blood pressure control, smoking cessation, and statin use.
To overcome the lack of power of these trials, an updated meta-analysis was conducted, pooling all available studies from 1988 through 2014, which replicated the finding of marginal benefit of aspirin reported in the ATC analysis. Yet the results were mainly driven by studies published before 2005, with no benefit found in the later trials.25,26
CONTEMPORARY TRIALS: THE TIEBREAKER?
Three recent clinical trials examined the role of aspirin for primary prevention of major cardiovascular events in a contemporary cohort of patients thought to be at higher risk of cardiovascular events in 3 distinct populations:
Patients at moderately elevated risk of cardiovascular events (estimated 10-year risk 10%-20%)8
Patients with diabetes9
The ARRIVE trial: No benefit in patients at low risk
The use of aspirin for primary prevention of cardiovascular events in those with elevated risk has been a point of heated debate in clinical practice.
The ASA to Reduce Risk of Initial Vascular Event (ARRIVE) trial8 was designed to clarify the benefit of aspirin in patients with an estimated 10-year risk of 10% to 20%. However, the actual rate of events was lower, at about 0.8% per year (or 8% in 10 years). Due to the low rate of events, the original primary end point (myocardial infarction, stroke, and cardiovascular death) had to be modified to include unstable angina and transient ischemic attack to adequately power the study.
The incidence of the primary composite end point and those of each component of the composite end point was no different between the aspirin and control groups. However, aspirin was associated with a significant reduction in myocardial infarction on per-protocol analysis. This finding must be interpreted with caution, given the potential for bias associated with a per-protocol analysis, although it provides an opportunity to explore the impact of aspirin in those that completed the intended intervention.
On the other hand, the use of aspirin was associated with a 2-fold higher rate of gastrointestinal bleeding (0.97% vs 0.46%, P = .0007), predominantly mild gastrointestinal bleeding. Approximately 1 gastrointestinal bleeding event would be caused by treating 196 patients for 10 years. Importantly, the incidence of bleeding was likely underestimated in this study, given the exclusion of patients perceived to be at higher risk of bleeding at enrollment.
In summary, this study found aspirin to have an unfavorable risk-benefit profile when used for primary prevention of cardiovascular events in a contemporary low-risk cohort. In this patient population, aspirin offers no adjunctive cardiovascular preventive benefit and moreover increases the risk of bleeding. Whether the cardiovascular benefit of aspirin in a higher-risk (> 10%-20% estimated 10-year risk) population without diabetes outweighs the bleeding risk remains unknown.
The ASCEND trial: Modest benefit in patients with diabetes
Preventive use of aspirin in patients with diabetes without established atherosclerotic cardiovascular disease has been another point of controversy. Patients with diabetes suffer a 2- to 3-fold higher rate of cardiovascular events, and they are thus thought to be a population that could benefit from preventive use of aspirin. Although earlier trials in patients with diabetes failed to demonstrate a definite benefit of aspirin in this group, these studies were grossly underpowered.
The larger Study of Cardiovascular Events in Diabetes (ASCEND) trial9 assessed the benefit of aspirin in men and women age 40 or older with diabetes and without atherosclerotic cardiovascular disease. Once again, the event rate was lower than anticipated, with an annual risk of 1.25% to 1.3% (or estimated 10-year risk of 12%-13%). As a result, the sample size and follow-up had to be increased, and the primary composite end point was modified to include transient ischemic attack to maintain the intended power.
Preventive use of aspirin resulted in an absolute reduction of 0.17% per year in the rate of the composite end point of nonfatal myocardial infarction, nonfatal stroke, transient ischemic attack, and vascular death (hazard ratio [HR] 0.88, 95% CI 0.79-0.97, P = .01). A total of 59 patients would need to be treated for 10 years to prevent 1 major cardiovascular event.
However, there was an absolute annual excess in major bleeding of 0.13% per year (HR 1.29, 95% CI 1.09-1.52, P = .003), which included gastrointestinal (62.3%), ocular (21.1%), intracranial (17.2%), and other site (20.4%) bleeds. Thus, 1 major bleeding event would be caused after treating 77 patients for 10 years. Thus, the use of low-dose aspirin in patients with diabetes (> 10% risk at 10 years) led to a modest reduction in cardiovascular events that was largely offset by an increase in major bleeding.
The ASPREE trial: Aspirin was harmful in the elderly
Similarly, the elderly are a population at increased risk of cardiovascular events that could, it was thought, profit from preventive use of aspirin.
The ASA in Reducing Events in the Elderly (ASPREE) trial sought to define the role of aspirin in those 70 years or older (or 65 or older if Hispanic or black) without established atherosclerotic cardiovascular disease and having a life expectancy longer than 5 years.10-12 Those with a clinical diagnosis of dementia, substantial physical disability, or high bleeding risk were excluded, as were those adhering to their medications less than 80% of the time during a run-in period. The main goal of the study was to determine if aspirin 100 mg daily would prolong a healthy life span in this population, using the composite end point of death, dementia, and persistent physical disability.
The study was stopped early due to futility after a mean follow-up of 4.7 years. There were no differences in the rates of the primary end point or individual secondary end points of cardiovascular events, dementia, or disability between the treatment groups.10,12
Worse, the use of aspirin translated into a net excess of 0.24% per year in major bleeding events (HR 1.38, 95% CI 1.18-1.62, P < .001), resulting in 1 major bleeding event after treating 42 patients for 10 years. Again, this risk is likely underestimated, given the exclusion of patients who could not tolerate aspirin during the run-in period. Aspirin increased the rates of upper gastrointestinal bleeds (HR 1.87, 95% CI 1.32-2.66) and intracranial hemorrhage of any kind (HR 1.50, 95% CI 1.11-2.02).
Surprisingly, a higher rate of all-cause mortality (HR 1.14, 95% CI 1.01-1.29 was noted in the aspirin group, mainly driven by cancer death, particularly colorectal cancers, challenging the theory that aspirin could prevent this type of cancer.
In summary, this contemporary primary prevention trial demonstrated a rather deleterious effect of aspirin in an unselected healthy elderly population (age > 70).
A new meta-analysis: Modest benefit, unacceptable risk
A 2019 meta-analysis27 summarized all available evidence, including the contemporary trials.
The use of aspirin for primary prevention of atherosclerotic cardiovascular disease was associated with a 0.3%-per-year reduction in the absolute risk of myocardial infarction but no benefit in reducing the risk of stroke or death, a very modest benefit that disappears when analyzing only studies published after 2008. Further, aspirin use in primary prevention is consistently associated with an absolute increase in the rates of intracranial bleeding at 0.1% per year and major bleeding at 0.2% per year.27
Overall, the use of aspirin appears harmful when prescribed for primary prevention of cardiovascular events in lower-risk patients without diabetes and unselected healthy elderly populations (age > 70). In patients without diabetes, a total of 265 patients need to be treated with aspirin for 10 years to prevent 1 cardiovascular event, while 1 major bleeding event would be caused after treating 210 patients.
On the other hand, patients with diabetes without atherosclerotic cardiovascular disease appear to enjoy a modest reduction in cardiovascular events when prescribed aspirin for primary prevention, although this benefit is largely counterbalanced by an increase in bleeding. About 153 diabetic patients would need to be treated for 10 years to prevent 1 major cardiovascular event, while treating 121 patients for 10 years would cause 1 major bleeding event.
Many questions remain regarding the use of aspirin for primary prevention of atherosclerotic cardiovascular disease. For instance it is still largely unknown whether it is justified in a higher-risk primary prevention cohort (> 20% estimated 10-year risk), or those with uncontrolled risk factors or risk enhancers such as coronary calcium, elevated lipoprotein(a), or elevated inflammatory markers.
PAST GUIDELINE UNCERTAINTIES AND CURRENT RECOMMENDATIONS
Major cardiovascular societies have interpreted the available evidence differently, leading to discrepant recommendations on the use of aspirin in primary prevention (Table 2).6,13,28-34
Aspirin for primary prevention: Recommendations from major societies
Earlier guidelines from the AHA/ACC, US Preventive Services Task Force (USPSTF), and American Diabetes Association supported the use of aspirin for primary prevention of cardiovascular events in those at high risk.28-32 The USPSTF and AHA/ACC used an estimated 10-year risk higher than 10% as a criterion for prophylactic initiation of aspirin. This recommendation was based on post hoc analysis of older trials that suggested with moderate certainty that the risk-benefit profile of aspirin was more favorable in those with an estimated 10-year risk greater than 10%, particularly in those age 50 to 59.
In contrast, the 2016 European Society of Cardiology guidelines6 advised against using aspirin for primary prevention, even before the 3 newer trials described above were published. This recommendation was based on a more direct interpretation of the evidence, acknowledging that even if aspirin conferred a very modest reduction in nonfatal cardiovascular events, this was largely offset by an increase in bleeding, with no decrease in mortality.
AHA/ACC 2019. Most recently, the AHA/ACC updated their recommendations,13 considering the evidence from the newer trials. The 2019 AHA/ACC guidelines recognized the greatly attenuated benefit of adjunctive aspirin in contemporary optimal medical management and acknowledged the systematic overestimation of risk with the use of pooled cohort equations. Hence, they downgraded the class of recommendation for prophylactic use of aspirin to class IIb (“it may be considered”) and removed any specific pooled cohort equation risk levels as criteria for recommending aspirin. In the new guidelines, prophylactic use of aspirin may be considered in selected adults age 40 to 70 at higher risk of atherosclerotic cardiovascular disease without a higher bleeding risk. In contrast, routine use of aspirin in healthy elders age 70 or older and in those at high bleeding risk is discouraged.
These more cautious recommendations highlight the lingering uncertainty about the impact of this intervention in those at the higher end of the cardiovascular risk spectrum such as those with uncontrolled risk factors despite optimal medical management, those with subclinical coronary atherosclerosis, and those with additional risk-enhancing factors such as elevated inflammatory markers or elevated lipoprotein(a).
Ultimately, the guidelines defer the decision to initiate aspirin for primary prevention to the patient-clinician encounter after weighing the risk vs the possible benefit in the patient in question and the totality of the evidence available.13
REMAINING GAPS IN KNOWLEDGE
As previously mentioned, most of the available evidence pertains to a low-risk primary prevention cohort, and no high-quality study has been conducted to assess the net risk-benefit profile of aspirin in selected young patients (age < 40) or in high-risk patients (> 20% 10-year risk) such as those with uncontrolled risk factors or risk enhancers. Therefore, great uncertainty remains about the potential impact of aspirin in selected young patients and those thought to be at the higher end of the risk spectrum.
Patients at high risk. Although a larger absolute benefit would be expected in those at higher baseline cardiovascular risk, it is also anticipated that the bleeding risk will increase, given the concomitant increase in bleeding associated with several cardiovascular risk factors such old age, diabetes, obesity, and smoking.30 Whether these risk factors increase cardiovascular disease and bleeding risk by the same magnitude remains unknown. Hence, the patient profile and the specific risk cutoff at which the primary prevention benefits of aspirin outweigh the bleeding risk remain unknown.
Another area of ambiguity relates to the proper classification (primary vs secondary prevention cohort) and subsequent management of patients without symptoms who are found incidentally to have atherosclerotic cardiovascular disease on coronary angiography or noninvasive imaging such as coronary artery calcium scoring or coronary computed tomographic angiography.
Coronary calcium. It is well known that the total burden of coronary plaque directly correlates with the rate of cardiovascular events. Such plaque burden can be easily estimated by measuring coronary artery calcium, with higher calcium scores resulting in proportional increment in cardiovascular risk.
Therefore, measuring coronary calcium greatly enhances the accuracy in estimating risk of cardiovascular events irrespective of age and comorbidities.35 For instance, patients with a calcium score greater than 100 experience cardiovascular events at a rate close to that in a stable secondary prevention population, while those with extensive calcium (scores > 1,000) experience event rates that exceed the rates observed in secondary prevention trials.36,37 On the other hand, absence of coronary calcium (scores of 0) is equally helpful in establishing that patients are not at risk, which is particularly helpful in those with a borderline or intermediate risk estimation based on the pooled cohort equation.38
Evidence from the Multi-ethnic Study of Atherosclerosis (MESA)39 suggested that the coronary calcium score might be of value when deciding whether to start aspirin for primary prevention of cardiovascular disease in patients without diabetes. In this regard, the risk-benefit profile of aspirin appears favorable in those with a calcium score greater than 100, with the odds of preventing vascular events 2 to 4 times higher than the chance of causing a bleed. In contrast, aspirin seems harmful in those with a score of 0, with a chance of bleeding that is 2 to 4 times higher than the likelihood of preventing a vascular event, regardless of traditional risk factors.
Lipoprotein(a). Similarly, the utility of lipoprotein(a) to ascertain the benefit of aspirin for the primary prevention of cardiovascular events remains uncertain. In a substudy from the Women’s Health Study,40 an elevated lipoprotein(a) was associated with a 2-fold higher rate of cardiovascular events, which was effectively attenuated by the use of aspirin.
High-quality studies are needed to define the role of coronary calcium and lipoprotein(a) in the decision to start aspirin for primary prevention of atherosclerotic cardiovascular disease in patients both with and without diabetes.
Aspirin dose. The optimal aspirin dose for primary prevention events remains uncertain. The current understanding is that low doses (75-100 mg per day) are effective in preventing vascular events while minimizing bleeding rates. On the other hand, the impact of statins and proton-pump inhibitors on the risk-benefit profile of aspirin in primary prevention remains unresolved.41 Further studies are needed to evaluate the optimal aspirin dosing. The upcoming ASA and Simvastatin Combination for Cardiovascular Events Prevention Trial (ACCEPT-D) is set to evaluate the strongly suspected attenuation effect of statins on the aspirin benefit.42
FROM THE EVIDENCE TO THE PATIENT
The decision to defer or prescribe aspirin in clinical practice for primary prevention of cardiovascular events remains a challenging one and should be individualized. It is important to first emphasize that primary prevention recommendations only apply to those patients without established atherosclerotic cardiovascular disease, namely no prior myocardial infarction, no prior ischemic stroke, no symptomatic peripheral arterial disease, and no prior coronary revascularization. In patients with these conditions, ie, the secondary prevention cohort, the benefit of aspirin is well established.
Primary prevention should always begin with encouragement of healthy life habits and optimal management of cardiovascular risk factors including weight loss, glucose and blood pressure control, and lipid management, per preventive guideline recommendations.13
The risk of atherosclerotic cardiovascular disease should be estimated using the pooled cohort equation in every patient before deciding on the prophylactic use of aspirin. In the new guidelines, patients are classified into 4 risk categories based on the pooled cohort equation13:
Low risk (10-year risk < 5%)
Borderline risk (5% to < 7.5%)
Intermediate risk (7.5% to < 20%)
High risk (> 20%).
Of importance, the current risk estimation tools (including the 10-year pooled cohort equation) systematically overestimate risk. Hence, incorporation of risk enhancers (eg, positive family history, elevated inflammatory markers, elevated lipoprotein(a), coronary calcium) could further refine the accuracy of the risk estimation and guide the escalation of preventive measures in selected cases. Although the use of such risk enhancers was mainly designed to guide statin therapy, they may also guide the decision to initiate aspirin in primary prevention, particularly coronary calcium and lipoprotein(a) based on available data as described above (Figure 1).
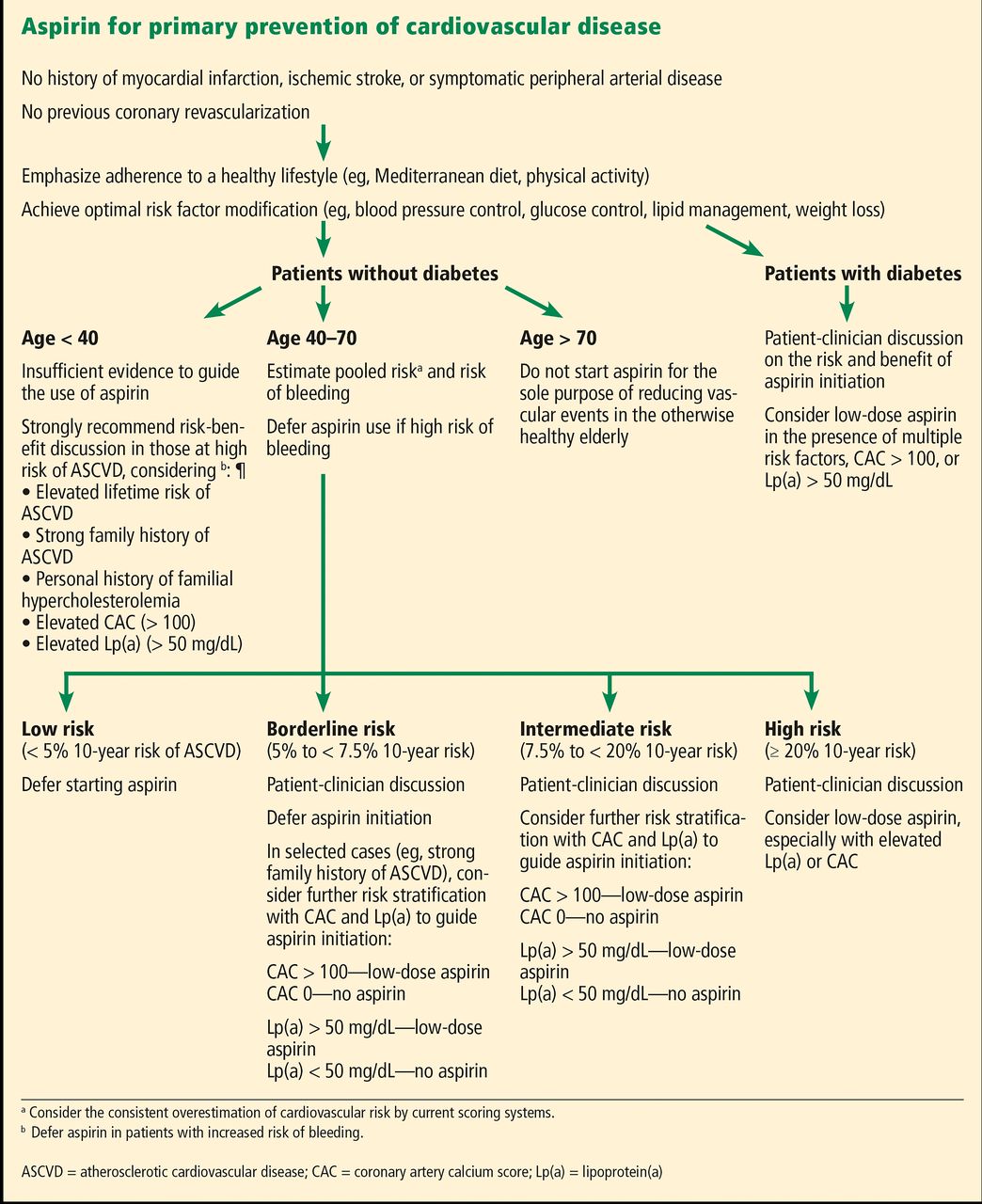
Our recommendations for aspirin use for primary prevention of cardiovascular events.
Ultimately, a preventive regimen of aspirin must reduce the rate of cardiovascular events by an absolute magnitude that is clinically meaningful, emphasizing the focus on treating those patients at the higher end of the cardiovascular risk spectrum.
It is equally important to estimate the risk of bleeding when considering primary preventive use of aspirin. Such risk might vary among patients based on age, concomitant medications, and comorbidities.5 The use of aspirin in primary prevention confers a 1.0% risk of bleeding over a 5-year period in men and a 1.1% risk in women. Age, smoking history, and diabetes, as well as a history of previous bleeding, peptic ulcer disease, cancer, and use of nonsteroidal anti-inflammatory drugs are associated with a further increase in the risk of bleeding.43 Similarly, it is well established that concomitant use of aspirin and anticoagulation is associated with a significant increase in bleeding with no ischemic benefit in a wide range of scenarios including primary prevention and atrial fibrillation.44,45
In summary, giving aspirin for primary prevention is to be considered only when the estimated cardioprotective effects of aspirin outweigh the bleeding risk on therapy.
The following recommendations are meant to provide a general guidance on the use of aspirin in clinical practice. However, the ultimate decision on whether to start or defer aspirin for primary prevention must be shared, considering the individual risk-benefit profile and the preferences of the patient at hand.
The use of aspirin for the sole purpose of primary prevention is discouraged in healthy elderly patients (age > 70) and those at high risk of bleeding, including patients on anticoagulation.
Similarly, routine use of aspirin for the sole purpose of primary prevention is best deferred in patients at low risk (< 5% 10-year risk) and borderline risk (5%-7.5% 10-year risk). In selected cases in patients at borderline risk such as those with a strong family history, clinicians could also consider risk enhancers such as coronary calcium in the discussion about the risks and benefits of starting aspirin.
A shared decision to initiate aspirin in those at intermediate risk (7.5%-20% 10-year risk) could be considered for patients with risk enhancers such as an elevated coronary calcium score (> 100) or elevated lipoprotein(a) (> 50 mg/dL).
In patients ages 40 to 70 at high risk of atherosclerotic cardiovascular disease (> 20% at 10 years), it is reasonable to consider starting low-dose aspirin as a shared decision if the patient is thought to be at low risk of bleeding.
Finally, scarcity of data in those younger than 40 precludes any recommendation to guide the use of aspirin in this population. A shared decision on the benefit of aspirin in younger patients (age < 40) is recommended in selected cases at high risk of atherosclerotic cardiovascular disease based on an elevated lifetime risk, strong family history, familial hypercholesterolemia, elevated coronary calcium score, or elevated lipoprotein(a).
Patients with diabetes are a unique population at higher risk of cardiovascular events. Again, risk factor modification is the first step for primary prevention of cardiovascular disease in this population, including glucose control favoring medications with proven cardiovascular benefit. Patientclinician risk discussion is strongly recommended to decide on the added value of starting aspirin in patients with diabetes, weighing perceived benefits against risks to the patient at hand. It is best to defer aspirin use in those at high risk of bleeding, while starting aspirin is reasonable in those patients with diabetes with multiple additional risk factors or who have risk enhancers such as a coronary calcium score higher than 100 and elevated lipoprotein(a).
CONCLUSION
Despite the large amount of data, the role of aspirin in contemporary practice for primary prevention of cardiovascular disease remains debatable. In contrast to the modest benefit reported by older trials, the most recent trials largely challenged the benefit of aspirin in current practice. This is in great part explained, as anticipated, by improved best preventive practices (eg, blood pressure control, lipid management with statins, smoking cessation) that dilute the potential benefit from aspirin for primary prevention.46
Nonetheless, the existing evidence mainly comes from low-risk populations and fails to definitively ascertain the impact of aspirin in those at higher risk of cardiovascular disease. If aspirin use is to be considered for primary prevention, it must remain limited to selected patients at elevated risk of cardiovascular disease but low risk of bleeding. The use of risk enhancers such as elevated coronary calcium scores and elevated lipoprotein(a) may be useful to accurately identify such patients at the higher end of the risk spectrum.
Further studies are needed to determine the primary prevention subgroups that would benefit from low-dose aspirin.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}