


Article Figures & Data
Figures
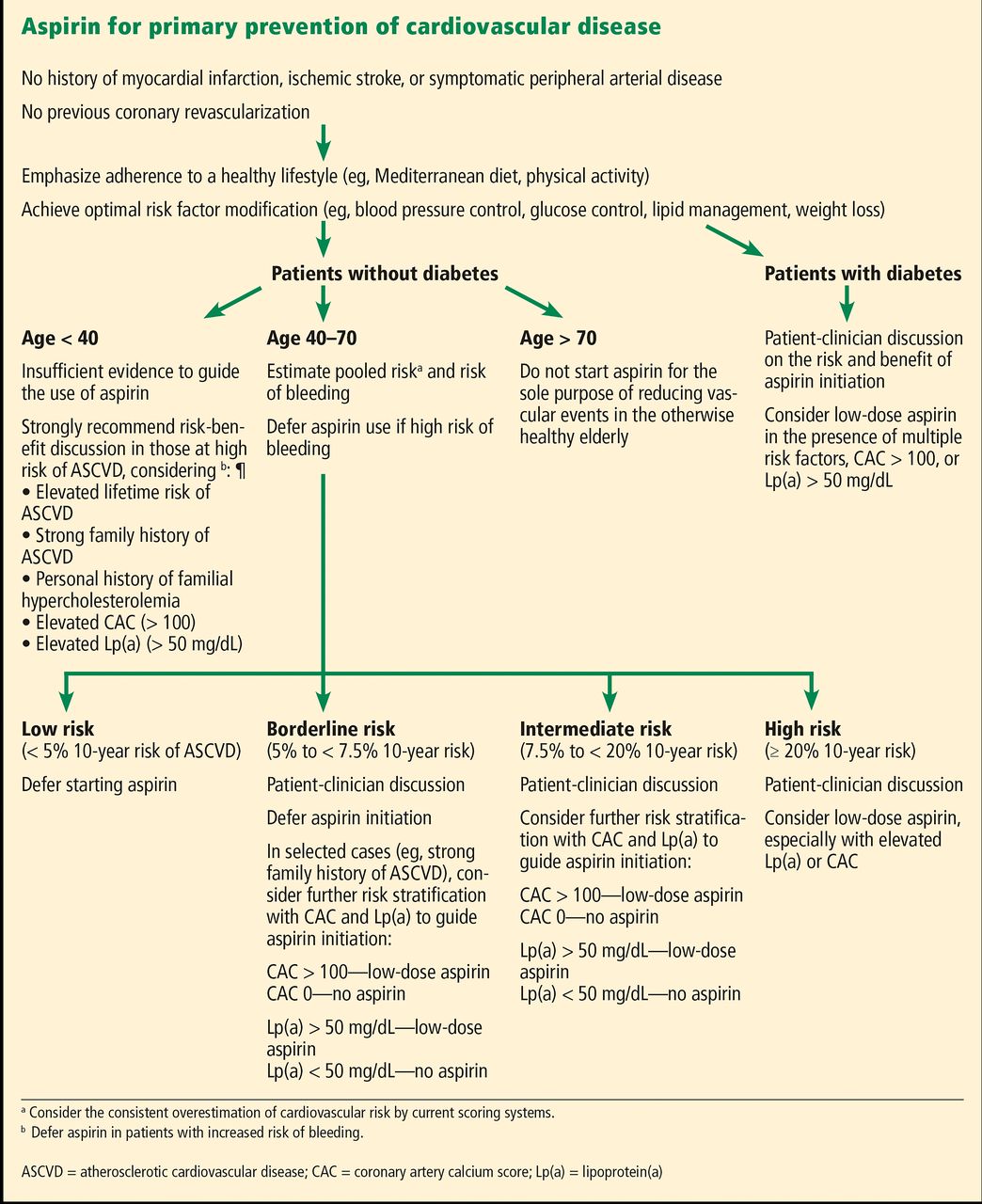
- Figure 1
Our recommendations for aspirin use for primary prevention of cardiovascular events.
Tables
Trial Year Population Number needed to treat or harma Nonfatal myocardial infarction Nonfatal ischemic stroke Major gastrointestinal bleed BDS14 1988 5,139 healthy male physicians [143] [250] ND PHS15 1989 22,071 healthy male physicians 67 [333] [250] TPT16 1998 5,085 men at high risk 40 125 [250] HOT17 1998 18,790 people with hypertension 77 1,000 [71] PPP19 2003 4,495 people with risk factors 143 250 333 WHS18 2005 39,876 healthy female nurses ND 500 1,000 POPADAD21 2008 1,276 people with diabetes, ABI < 0.99 500 36 143 JPAD23 2008 2,539 people with diabetes [167] 1,000 [200] AAA24 2010 3,350 people with ABI < 0.91 200 1,000 [1,000] JPPP22 2014 14,000 people with > 1 risk factor 250 ND [50] ARRIVE8 2018 12,526 men with 2-4 risk factors or women with > 3 risk factors 333 333 [100] ASCEND9 2018 15,480 people with diabetes 1,000 333 [167] ASPREE10-12 2018 19,114 healthy elderly 333 250 42 ↵a The number of patients who would need to be treated for 10 years to prevent or cause 1 event, calculated as the inverse of the absolute difference in the proportion of patients with events per year between the aspirin and placebo groups. Numbers in brackets indicate harm, ie, higher rates in the aspirin group.
AAA = Aspirin for Asymptomatic Atherosclerosis; ABI = ankle-brachial index; ASCEND = A Study of Cardiovascular Events in Diabetes; ASPREE = A Study of Cardiovascular Events in Diabetes (ASCEND) and Aspirin in Reducing Events in the Elderly; ARRIVE = Aspirin to Reduce Risk of Initial Vascular Events; BDS = British Doctors Study; HOT = Hypertension Optimal Treatment; JPAD = Japanese Primary Prevention of Atherosclerosis With Aspirin for Diabetes; JPPP = Japanese Primary Prevention Project; ND = no difference; PHS = Physicians’ Health Study; POPADAD = Prevention of Progression of Arterial Disease and Diabetes; PPP = Primary Prevention Project; TPT = Thrombosis Prevention Trial; WHS = Women’s Health Study
American Heart Association/American College of Cardiology, 20027 Low-dose aspirin recommended in persons at higher cardiovascular risk, especially those with 1-year risk > 10% Low-dose aspirin recommended in patients with diabetes at increased cardiovascular risk, including those who are over age 40 or who have additional risk factors Therapy should not be recommended for patients with diabetes under age 21 because of the increased risk of Reye syndrome associated with aspirin use in this population; patients with diabetes under age 30 have not been studied European Society of Cardiology, 20166 Antiplatelet therapy is not recommended in individuals without cardiovascular disease due to the increased risk of major bleeding Antiplatelet therapy (eg, aspirin) is not recommended for people with diabetes who do not have cardiovascular disease US Preventive Services Task Force, 201734 Low-dose aspirin is recommended in adults ages 50-59 who have a > 10% 10-year risk, are not at increased risk for bleeding, have a life expectancy of > 10 years, and are willing to take it daily for > 10 years The decision to initiate low-dose aspirin for primary prevention of cardiovascular disease and colorectal cancer in adults ages60-69 who have a 10% or greater 10-year cardiovascular disease risk should be an individual one The current evidence is insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of cardiovascular disease and colorectal cancer in adults under age 50 The current evidence is insufficient to assess the balance of benefits and harms of initiating aspirin use for primary prevention of cardiovascular disease and colorectal cancer in adults age 70 or older American Academy of Family Physicians, 201633 Low-dose aspirin use for primary prevention of cardiovascular disease and colorectal cancer is recommended in adults ages 50-59 who have a 10% or greater 10-year cardiovascular disease risk, are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose aspirin daily for at least 10 years The decision to initiate low-dose aspirin use for the primary prevention of cardiovascular disease and colorectal cancer in adults ages 60-69 who have a 10% or greater 10-year cardiovascular disease risk should be an individual one Evidence is insufficient to assess risk-benefit profile of aspirin for primary prevention of cardiovascular disease and colorectal cancer in adults younger than 50 The current evidence is insufficient to assess the balance of benefits and harms of starting aspirin for primary prevention of cardiovascular disease and colorectal cancer in adults age 70 or older American Diabetes Association, 201832 Low-dose aspirin may be considered as a primary prevention strategy in those with type 1 or type 2 diabetes who are at increased cardiovascular risk; this includes most men and women with diabetes age > 50 who have at least 1 additional major risk factor and are not at increased risk of bleeding American Heart Association/American College of Cardiology, 201913 Low-dose aspirin might be considered for the primary prevention of atherosclerotic cardiovascular disease (ASCVD) among select adults ages 40-70 who are at higher ASCVD risk but not at increased bleeding risk Low-dose aspirin should not be prescribed on a routine basis for primary prevention of ASCVD among adults age > 70 Low-dose aspirin should not be prescribed for primary prevention of ASCVD among adults of any age who are at increased risk of bleeding




{kind=link}