


A 30-year-old man presented with a 6-month history of an exophytic mass growing on the lower mid-back (Figure 1). It was initially suspected to be verruca vulgaris, and he had been referred to a specialty clinic for sexually transmitted infections to confirm it. The lesion was occasionally tender to palpation and bled spontaneously.

A solitary ulcerated, purple-red polypoid nodule with overlying serous crust on the lower mid-back.
Physical examination revealed a 1.5-cm ulcerated, violaceous-to-erythematous polypoid nodule with overlying serous crust on the lower back. No pigmentation was noted within the mass or adjacent to the base of the lesion.
Histopathologic examination of a shave biopsy specimen revealed:
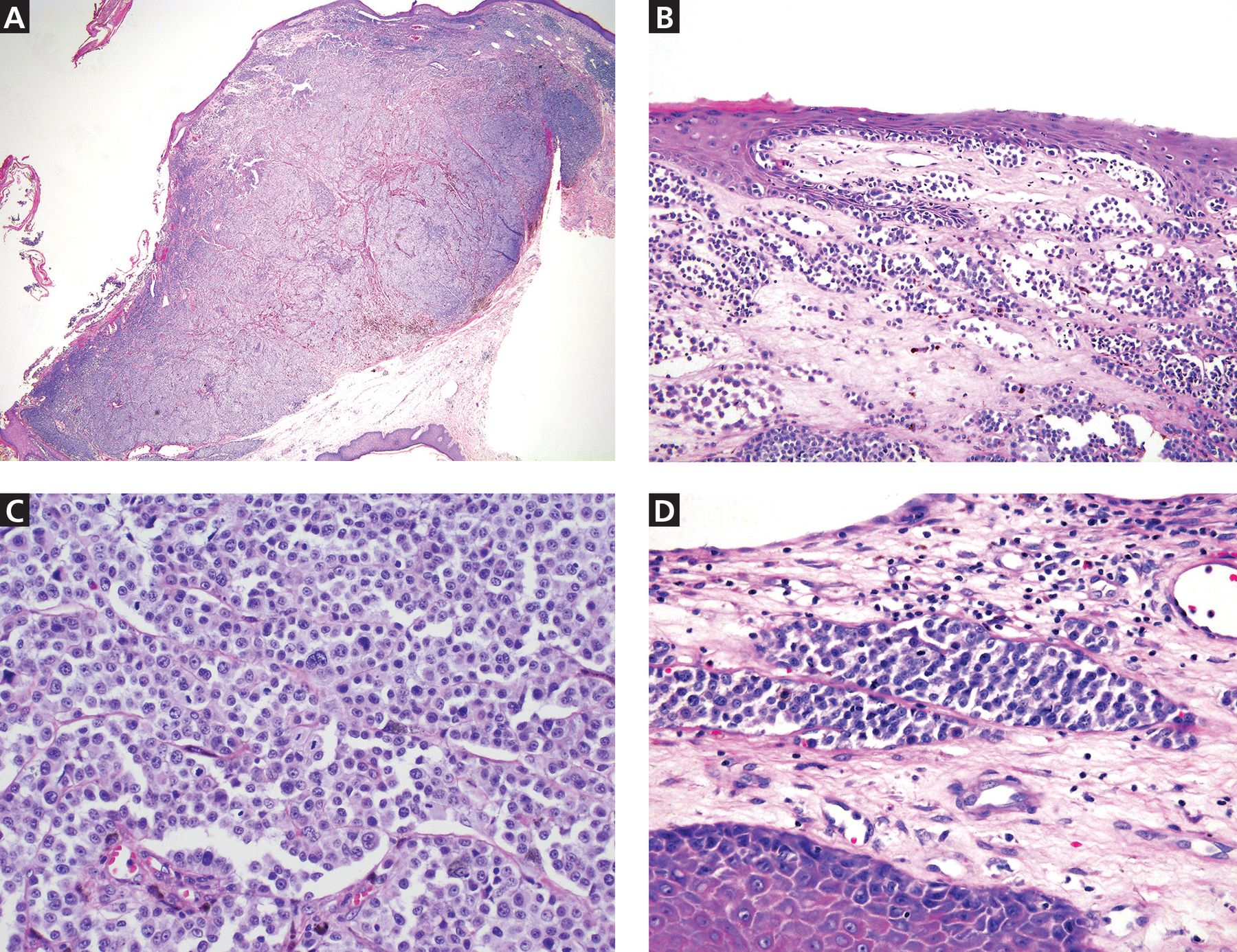
An exophytic polypoid lesion with broad ulceration, composed of markedly atypical melanocytes in a sheet-like pattern throughout the dermis (Figure 2A)
Focal epidermal contiguity with atypical melanocytes arranged in single cells and nests in the epidermis (Figure 2B)
A mitotic rate of greater than 30 mitoses/mm2 (Figure 2C)
Lymphovascular invasion (Figure 2D)
Melanocytes highlighted by S-100 protein on immunohistochemical staining.

Histopathologic images show (A) an exophytic polyp with ulceration and atypical melanocytes arranged in a sheet-like pattern throughout the dermis (hematoxylin and eosin [H&E] stain, original magnification × 2) and (B) focal epidermal contiguity with atypical melanocytes arranged in single cells and nests in the epidermis (H&E stain, original magnification × 20). High-power images (H&E stain, original magnification × 40) show (C) confluent, atypical melanocytes with conspicuous mitoses and focal cytoplasmic melanin, and (D) lymphovascular invasion at the periphery of the lesion.
These findings were diagnostic of melanoma, specifically the polypoid variant, with a tumor thickness of 5 mm.
The patient was referred for wide local excision with sentinel lymph node biopsy, which demonstrated inguinal node involvement and BRAF mutation on immunostaining. Positron-emission tomography–computed tomography, magnetic resonance imaging, and computed tomography of the head, chest, abdomen, and pelvis were unrevealing. The formal diagnosis was stage IIIC disease (T4bN1M0). The patient began immunotherapy with nivolumab. He was treated with this drug for 1 year and now is on active surveillance.
IMPORTANCE OF ACCURATE DIAGNOSIS
Polypoid melanoma is a rare clinical variant of nodular melanoma characterized by an exophytic mass with frequent ulceration, young age at onset (20 to 39 years), and poor prognosis.1,2 It has been reported to account for 2% to 43% of all melanomas, with the wide variability attributed to discrepancies in clinicopathologic criteria used in different reports.1
Lesions can affect the mucosa of the upper respiratory tract, esophagus, and anorectal junction, although cutaneous lesions are most frequently on the back.2–5 Polypoid melanomas have a propensity for ulceration, rapid progression over several weeks to months, and early metastasis to the lymph nodes, followed by possible metastasis to distant sites such as the skin, brain, liver, and subcutaneous soft tissue.2,4
Of the melanoma variants, polypoid melanoma has the poorest prognosis, given the risk of regional lymphatic and distal micro-metastatic involvement, often attributed to increased tumor thickness and ulceration at presentation.2–4 The 5-year survival rate for the polypoid nodular variant ranges from 32% to 42%, compared with 57% for nonpolypoid nodular melanoma and 77% for superficial spreading melanoma.2,5
Potential for misdiagnosis
Polypoid melanoma is often misdiagnosed, as it may be confused with benign skin conditions such as verruca vulgaris, leading to inappropriate treatment with cryotherapy or electrodessication and curettage. Other conditions to consider in the differential diagnosis include pyogenic granuloma, keratoacanthoma, and infarcted intradermal nevi or acrochordons, as these lesion types may similarly present with small protruding or dome-shaped papules.
Although these lesions often have distinguishing features, such as central hyperkeratosis in keratoacanthomas or the characteristic collarette of acanthotic epidermis at the base of pyogenic granulomas, polypoid melanomas may still be difficult to diagnose clinically, given that both pedunculated and sessile forms exist, as well as both pigmented and amelanotic variants. Additionally, ulceration may have many causes and can be seen in both benign and malignant growths. It may also obscure clinical presentation of cutaneous neoplasms, and tissue biopsy with histopathologic review should be considered for diagnostic guidance in such cases.
Given the highly aggressive clinical behavior and poor prognosis of polypoid melanoma, clinicians should maintain a low threshold for removal of rapidly growing pedunculated lesions with histopathologic evaluation, especially if the patient is relatively young and the lesion has progressed quickly or has ulcerated.
MANAGEMENT
Because polypoid melanoma may closely mimic benign lesions, patients with suspect lesions should be referred to dermatology for evaluation and biopsy as soon as possible. If timely dermatologic care is unavailable, priority should be given to biopsy techniques yielding adequate material for histopathologic analysis, such as a shave biopsy. Destructive treatments such as cryotherapy, used to manage benign lesions with similar appearances, should be avoided, as inappropriate treatment may delay accurate diagnosis and management.
Management of polypoid melanoma begins with prompt surgical excision. If it is not diagnosed early, sentinel lymph node biopsy and imaging studies may be needed to assess for disease progression. Additional therapy depends on extent of the disease and can include immunotherapy with immune checkpoint inhibitors or targeted therapy, such as BRAF and MEK inhibitors.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.