


Article Figures & Data
Figures
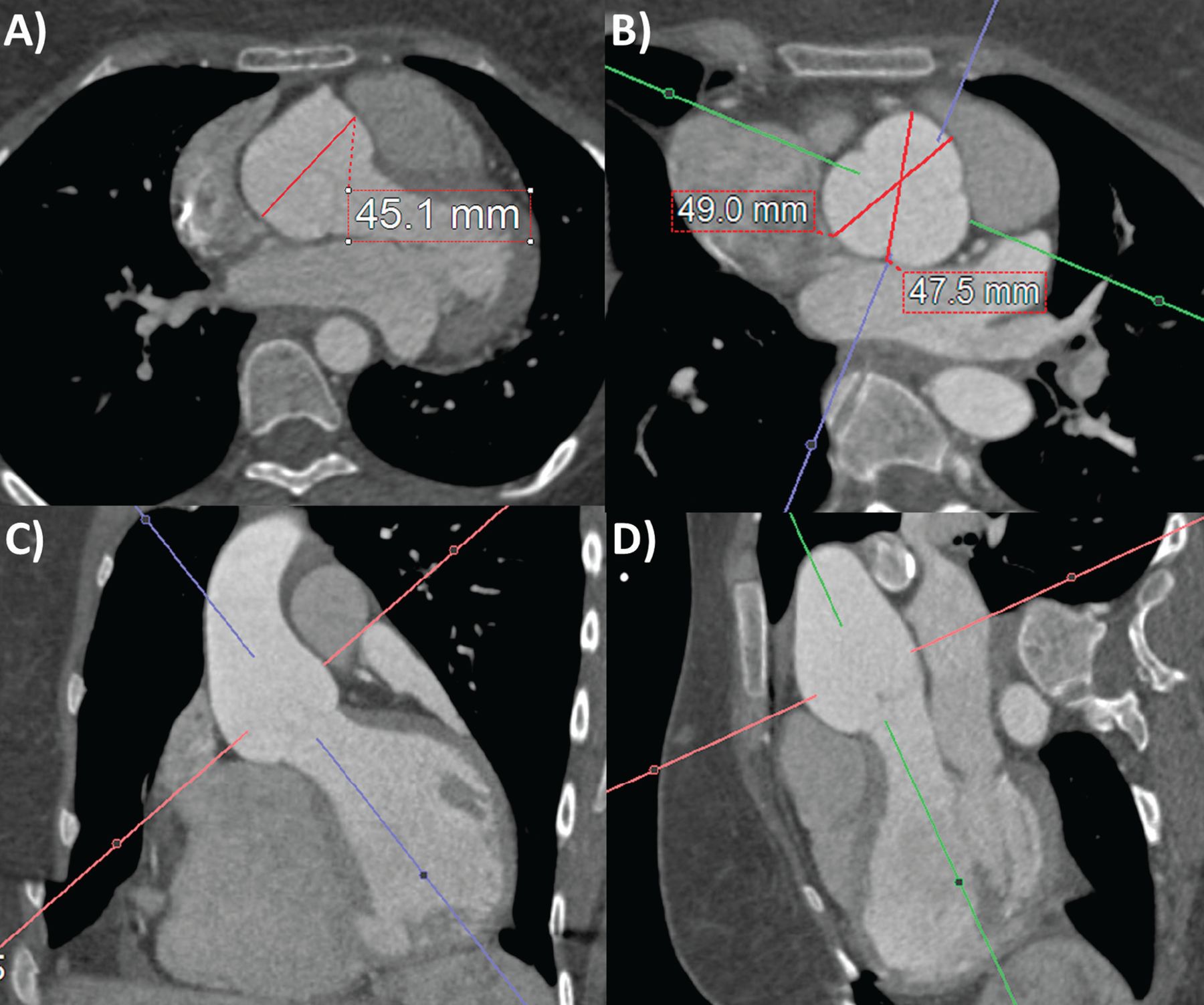
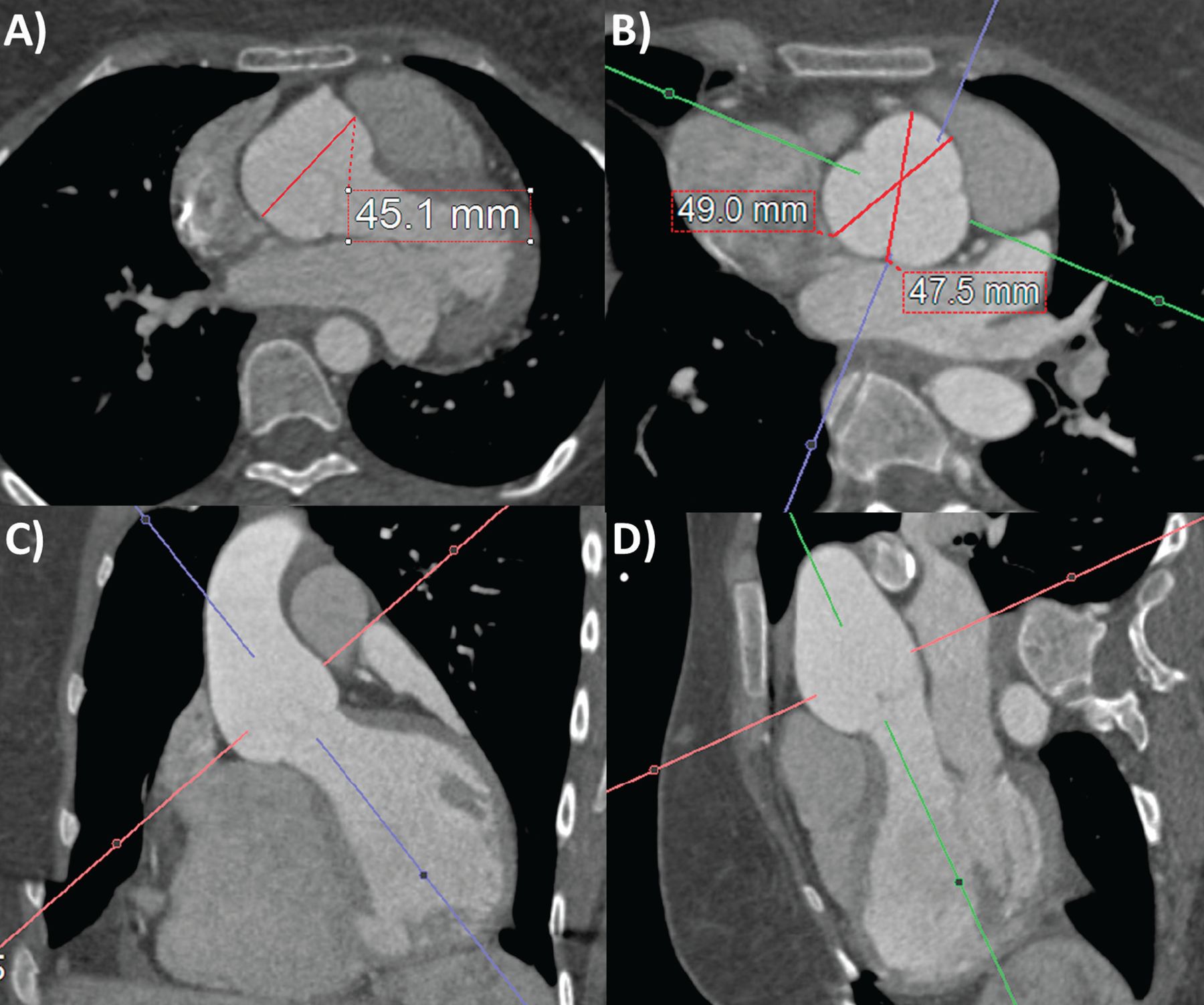
- Figure 1
Computed tomography angiography aortic root measurements on (A) axial source image and (B–D) 3-dimensional multiplanar reconstruction (3-D-MPR) double-oblique planes. Note that without 3-D-MPR, the aortic root size is underestimated (A). Also note that sinus-commissure measurements are often slightly less than sinus-sinus measurements in (B).
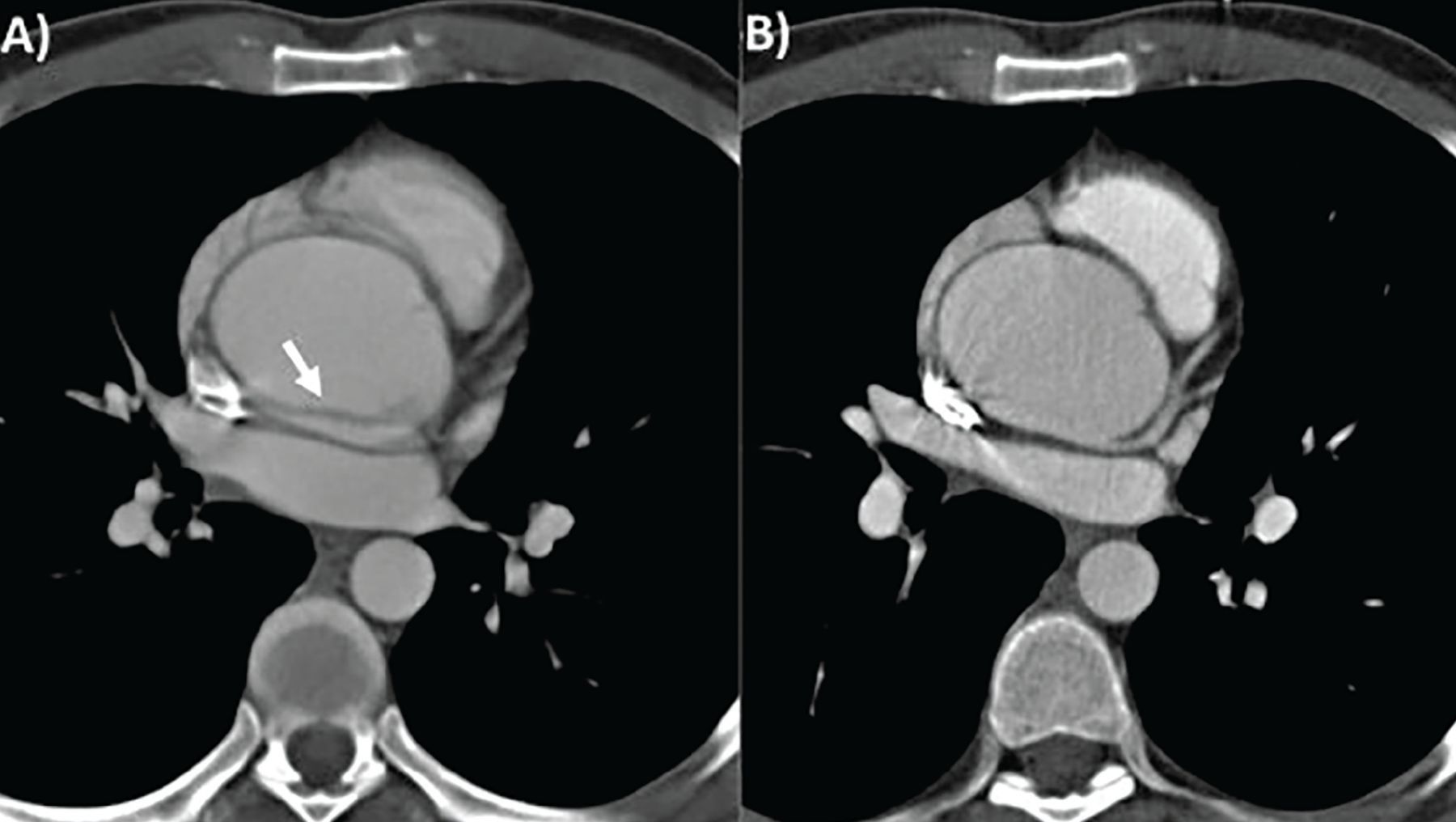
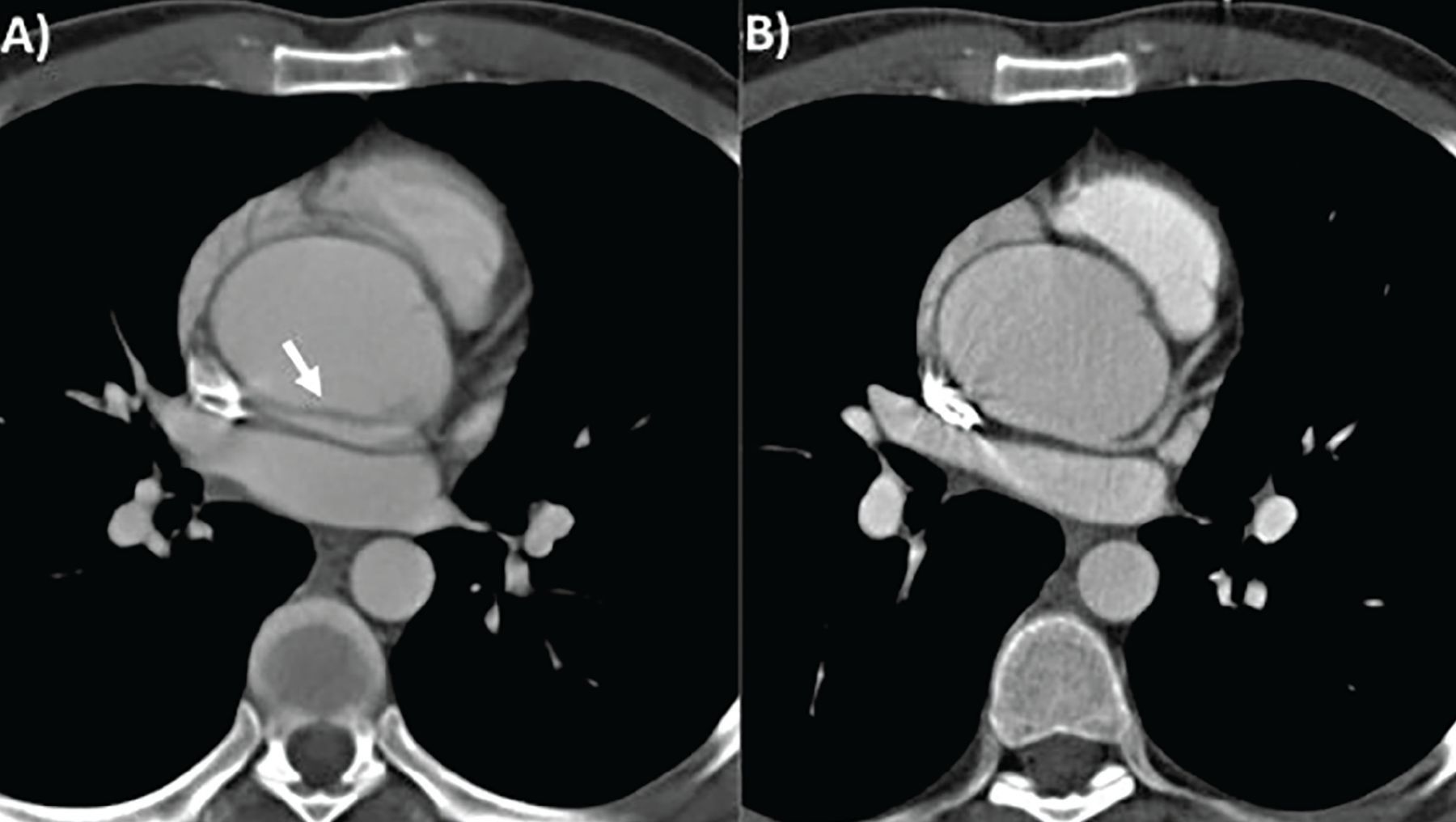
- Figure 2
Computed tomography of thoracic aortic aneurysm without (A) and with (B) electrocardiographic gating. Note that the motion artifact indicated by the white arrow in (A) is not seen in (B).
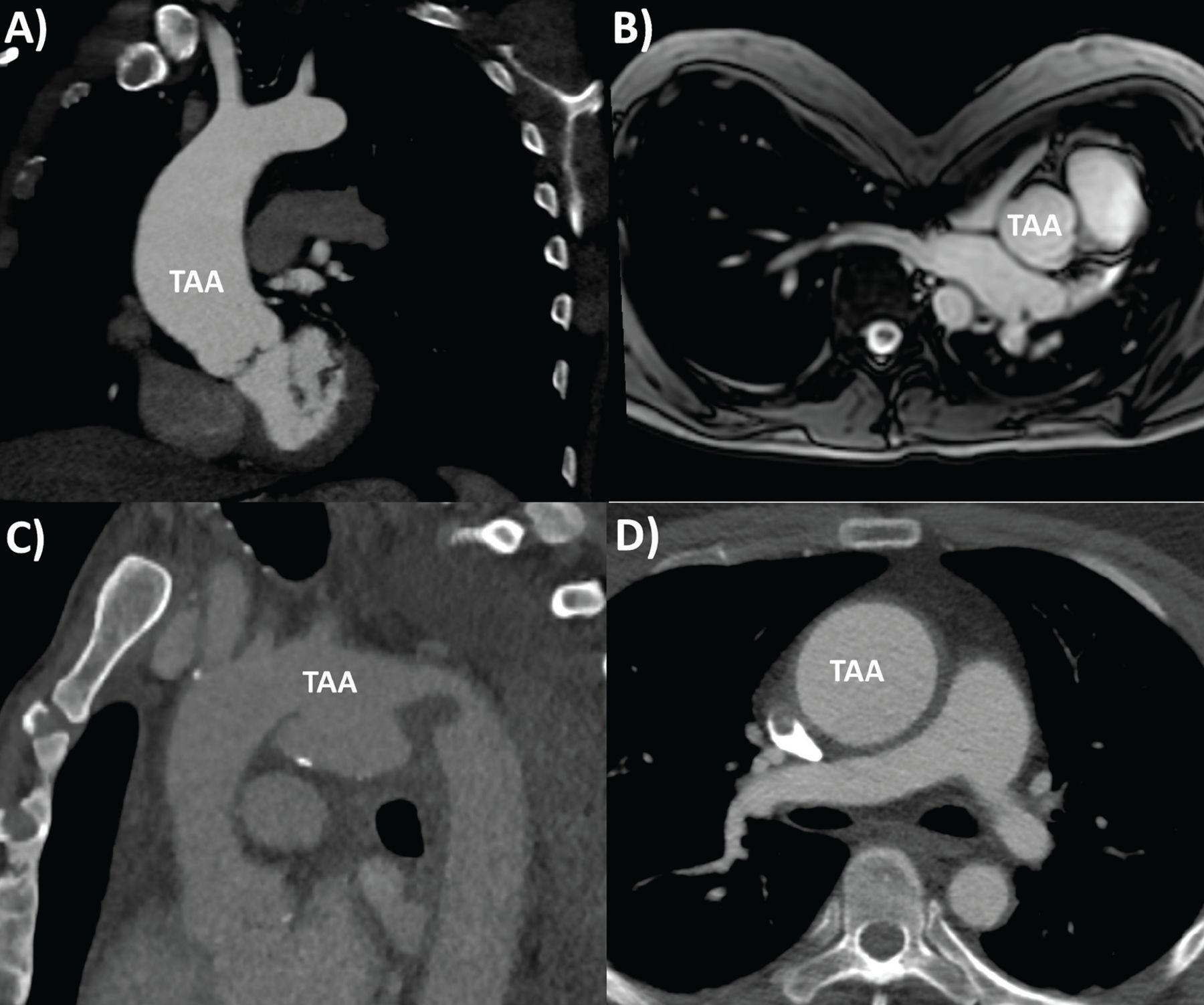
- Figure 3
Range of thoracic aortic aneurysm (TAA) pathologies: (A) bicuspid aortic valve aortopathy on computed tomography (CT), (B) Marfan syndrome with pectus excavatum on magnetic resonance imaging, (C) mycotic aortic arch aneurysm on CT, (D) Takayasu arteritis on CT, with thickened, inflamed aortic wall.
- Figure 4
Cross-sectional area-to-height ratio and management-stratification Kaplan-Meier survival curves for (A) aortic root and (B) ascending aorta in 969 consecutive patients with bicuspid aortic valve with proximal aorta diameter ≥ 4 cm, who underwent gated contrast-enhanced thoracic computed tomography or magnetic resonance angiography. Note the worse outcomes for those with aortic root area-to-height ratio > 10 cm2/m, in whom surgery makes a big difference in survival.
Reprinted from Masri A, Kalahasti V, Svensson LG, et al. Aortic cross-sectional area/height ratio and outcomes in patients with bicuspid aortic valve and a dilated ascending aorta. Circ Cardiovasc Imaging 2017; 10(6):e006249. doi:10.1161/CIRCIMAGING.116.00624


Tables
Risk factors Older age Male sex Hypertension Smoking Hypercholesterolemia Weight-lifting Cocaine use Trauma Cardiovascular associations Atherosclerosis Bicuspid aortic valve Other aneurysm Prior aortic dissection Aortic coarctation Genetic causes Familial thoracic aortic aneurysm Marfan syndrome Loeys-Dietz syndrome Ehlers-Danlos syndrome Turner syndrome Autosomal-dominant polycystic kidney disease Shprintzen-Goldberg (craniosynostosis) syndrome Inflammatory causes Takayasu arteritis Giant-cell arteritis Behçet arteritis Ankylosing spondylitis Infective causes Mycotic aortitis Syphilis Idiopathic Considerations TTE TEE CTA MRA Aortography Accuracy of measurement Medium Medium High High Low Extent of aortic assessment Limited Medium Entire Entire Limited Detecting acute aortic syndromes Poor Medium High High Poor Aortic regurgitation and grading Yes Yes No Yes Limited Portable Yes Yes No No No Contrast No No Yes Yes Yes Radiation No No Yes No Yes Cost Low Medium Medium High High Invasive procedure No Yes No No Yes Recommended line of investigation Second Third First Second Third CTA = computed tomography angiography; MRA = magnetic resonance angiography; TEE = transesophageal echocardiography; TTE = transthoracic echocardiography
Based on information in reference 9.
Aneurysm location and associated conditions ACC/AHA 20102 ESC 20141 Our recommendation Ascending aorta
No associated conditions
≥ 5.5 cm (I-C)a
≥ 0.5 cm/year growth (I-C)
≥ 5.5 cm (I-C), lower if small stature, rapid progression, aortic regurgitation (AR), pregnancy, patient preference (IIa-C)
≥ 5.5 cm
π r2/H > 10Aortic valve surgery planned > 4.5 cm (I-C) > 4.5 cm > 4.5 cm Marfan syndrome 4.0–5.0 cm (I-C)
π r2/H > 10 (IIa-C)≥ 5.0 cm (I-C)
> 4.5 cm with risk factors or family history (IIa-C)
≥ 0.3 cm/year growth, severe AR, pregnancy desired (IIa-C)> 4.5 cm
π r2/H > 10Bicuspid aortic valve ≥ 4.0–5.0 cm (I-C)
π r2/H > 10 (IIa-C)≥ 5.5 cm without risk factors (I-C)
≥ 5.0 cm with risk factors, family history, hypertension, aortic coarctation (I-C)
≥ 4.5 cm if AVR planned (I-C)
≥ 0.3 cm/year growth (IIa-C)≥ 5.0 cm without risk factors
≥ 4.5 cm with risk factors
π r2/H > 10Turner syndrome 4.0–5.0 cm (I-C)
π r2/H > 10 (IIa-C)Indexed aortic diameter ≥ 27.5 mm/m2 ≥ 27.5 mm/m2
π r2/H > 10Loeys-Dietz syndrome (apply to TGFBR1 or TGFBR2 mutation) ≥ 4.2 cm (TEE) (IIa-C)
≥ 4.4–4.6 cm (CTA/MRA)
(IIa-C)≥ 5.0 cm (I-C)
≥ 4.5 cm with risk factors (IIa-C)≥ 4.5 cm
π r2/H > 10Ehlers-Danlos syndrome 4.0–5.0 cm (I-C)
π r2/H > 10 (IIa-C)No specific threshold recommended ≥ 4.5 cm
π r2/H > 10Familial TAA 4.0–5.0 cm (I-C)
π r2/H > 10 (IIa-C)No specific threshold recommended ≥ 4.5 cm
π r2/H > 10Aortic arch
None
≥ 5.5 cm (IIa-B)
≥ 5.5 cm (IIa-C)
Consider if having ascending or descending TAA surgery (IIa-C)
≥ 5.5 cmDescending aorta
Stent graft
≥ 5.5 cm (I-B)
≥ 5.5 cm (IIa-C)
≥ 5.5 cmSurgery ≥ 6.0 cm (I-C) (include high risk, thoracoabdominal) ≥ 6.0 cm (IIa-C) ≥ 6.0 cm Surgery with degenerative, traumatic or saccular TAA, or postoperative pseudo-aneurysm ≥ 5.5 cm (I-B) No specific threshold recommended ≥ 5.5 cm Surgery with connective tissue disorder like Marfan or Loeys-Dietz syndrome Lower threshold than > 6 cm (I-C) Lower threshold than > 6 cm ≥ 5.5 cm ↵a Class of recommendation (scale of I to III) and level of evidence (scale of A to C).
ACC = American College of Cardiology; AHA = American Heart Association; AVR = aortic valve surgery; CTA = computed tomographic angiography; ESC = European Society of Cardiology; MRA = magnetic resonance angiography π r2/H = maximal cross-sectional area of TAA divided by height; TAA = thoracic aortic aneurysm
Associated conditions ACC/AHA 20102 ESC 20141 ASE/EACVI 20153 Our recommendations None No specific recommendations except needing surveillance No specific recommendations except needing surveillance Every 1–3 years based on risk after diagnosis TTE and CTA or MRA at baseline and 6 months; If TAA < 5.0 cm and stable, then yearly
If TAA ≥ 5.0 cm or growing > 0.5 cm/year, then every 6 months and refer to surgeonMarfan syndrome Measure dimensions and maximum cross-sectional area divided by height
TTE at baseline and 6 months, CTA or MRA at baseline to check TTE
If stable and < 4.5 cm, then yearly after, if not then more frequentlyTTE and MRA or CTA
If no TAA at baseline, TTE yearly, MRA or CTA every 5 years
If any aneurysm is above root, MRA or CTA yearly
Refer to 2010 ESC adult congenital disease guidelines35Dimensions with normative values based on age, body surface area, and Z scores
TTE and CTA or MRA
If no TAA at baseline, then every 2–3 years
First TAA diagnosis: 6 months then yearly if stable, < 4.5 cm and no dissection history; otherwise every 6 months
Postoperatively: 6 months, then yearly if stable CTA or MRA at least every 3 years if using TTETTE and CTA or MRA at baseline
and 6 months
If no TAA, then TTE yearly and CTA or MRA every 2 years
First TAA diagnosis: TTE and CTA or MRA yearly if stable (< 0.3 cm/year) and < 4.5 cm, other-wise every 6 months and refer to surgeonBicuspid aortic valve No specific recommendations after initial imaging TTE and CTA or MRA TTE and CTA or MRA
If no TAA at baseline, repeat TTE yearly
If TAA > 4.5 cm or growing at > 3 mm/year, then do CTA or MRA to confirm at same time, then yearlyTTE and CTA or MRA
If no at baseline, repeat every 3–5 years
First TAA diagnosis: 6 months then yearly if stable, < 4.5 cm and no dissection history; otherwise every 6 months
Postoperatively: yearly but individualizeTTE + CTA or MRA at baseline and 6 months
No TAA: TTE yearly and CTA or MRA every 2 years
First TAA diagnosis: TTE and CTA or MRA yearly if stable (< 0.3 cm/year) and < 4.5 cm, other-wise every 6 months and refer to surgeonTurner syndrome Baseline TTE and CTA or MRA
If no TAA or dissection risk factors, repeat every 5–10 yearsIf no TAA: TTE every 3–5 years for low risk, MRA every 3–5 years for moderate risk, and MRI every 1–2 years for high risk Index dimensions by body surface area; if indexed diameter > 2 cm/m2, repeat yearly TTE + CTA or MRA at baseline and 6 months
Index dimensions by body surface area
No TAA: TTE yearly and CTA or MRA every 2 years
Indexed diameter > 2 cm/m2: yearly MRA or CTA and refer to surgeonFamilial TAA No specific recommendations after initial imaging TTE and CTA or MRA No specific recommendations after initial imaging TTE and CTA or MRA Follow plan for Marfan syndrome, but individualize TTE + CTA or MRA at baseline and 6 months
Follow plan for Marfan syndrome but individualize riskLoeys-Dietz syndrome Baseline and 6 months TTE and CTA or MRA, then yearly if stable
Whole-body MRANo specific recommendations after initial imaging TTE and CTA or MRA Every 1–3 years depending on risk, every 6 months if progression TTE + CTA or MRA at baseline and 6 months
Yearly if low risk, < 4.0 cm and stable (< 0.3 cm/year), otherwise every 6 months and refer to surgeonEhlers-Danlos syndrome No specific recommendations No specific recommendations, individualize No specific recommendations TTE + CTA or MRA at baseline and 6 months
No specific recommendation for surveillanceACC = American College of Cardiology; AHA = American Heart Association; ASE = American Society of Echocardiography;
CTA = computed tomography angiography; EACVI = European Association of Cardiovascular Imaging; ESC = European Society of Cardiology;
MRA = magnetic resonance angiography; MRI = magnetic resonance imaging; TAA = thoracic aortic aneurysm; TTE = transthoracic echocardiography
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- WHAT IS THE CLINICAL IMPORTANCE OF TAA?
- WHO IS AT RISK?
- HOW IS TAA DISCOVERED?
- WHAT IS A NORMAL-SIZE AORTA?
- WHAT IMAGING MODALITIES ARE USED?
- WHEN SHOULD TAA BE FIXED?
- HOW SHOULD TAA BE MONITORED?
- DO DRUGS SLOW THE RATE OF TAA EXPANSION?
- HOW SHOULD TAA BE FIXED?
- WHAT ELSE SHOULD BE MANAGED?
- REFERENCES
- Figures & Data
- Info & Metrics