


A 51-year-old man presented with a 3-month history of reddish-brown lesions on his body and scaly brown lesions on the palms and soles and a 1-month history of mildly painful oral erosions. He had also noticed a buzzing sound in the right ear for the past 20 days.
Review of his medical record showed that he had engaged in unprotected sexual contact with a commercial sex worker 1 year earlier. He had human immunodeficiency virus (HIV) infection and had been taking antiretroviral therapy consisting of zidovudine, lamivudine, and nevirapine for the last 10 years, and his CD4 cell count was 706/μL.
Cutaneous examination revealed well-defined dusky to erythematous papules and plaques on his face, neck, back, and hands. There were well-defined ulcers on the tip of the tongue and split papules on both angles of the mouth. There were discoid plaques with peripheral scales on the palms (Figure 1) and soles (Figure 2). Other mucosae were normal, as were the results of the nervous system and ophthalmologic examinations.

Well-defined dusky, discoid patches and plaques with peripheral collarette of scales (red arrows) on the palms.

Well-defined dusky, discoid plaques with peripheral desquamative scaling on the instep of the patient’s soles. Some of the lesions appear psoriasiform.
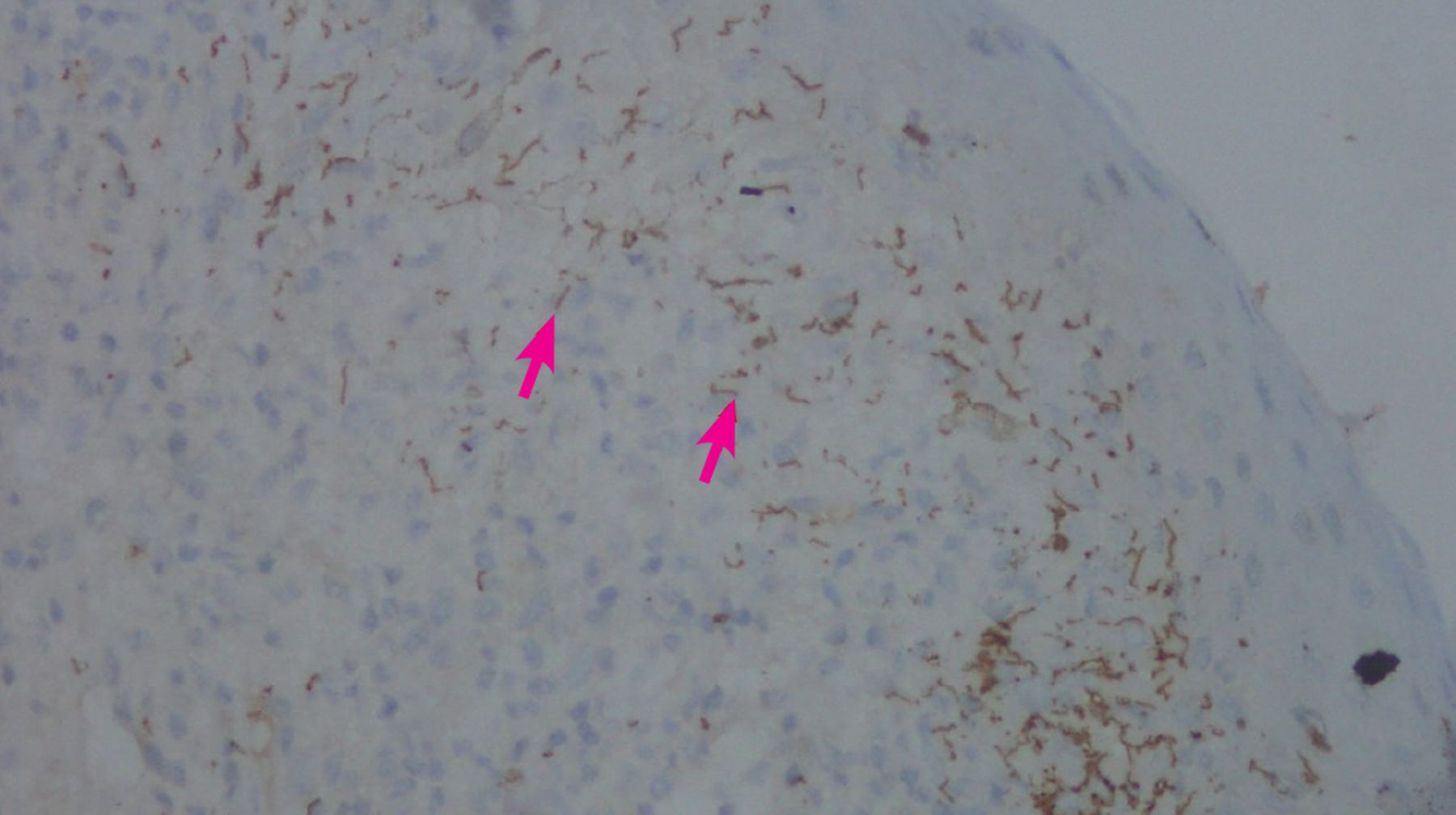
Skin biopsy of a cutaneous papule revealed dermis with periadnexal and perivascular plasma-cell-rich inflammatory infiltrate. Immunostain for Treponema further revealed helically coiled spirochetes present diffusely in the dermis (Figure 3).

Immunostain for Treponema showed helically coiled spirochetes, stained brown (red arrows), scattered throughout the dermis (magnification × 40).
A Venereal Disease Research Laboratory test (titres of 1:64) and Treponema pallidum hemagglutination assay were positive (titres of 1:80). Cerebrospinal fluid analysis was normal. However, tympanometry revealed a type C tympanogram with minimal sensorineural hearing loss in the right ear.
Based on these findings and the patient’s history, otosyphilis accompanying secondary syphilis was suspected. Owing to the unavailability of crystalline penicillin and procaine penicillin, intravenous ceftriaxone 2 g daily was administered for 14 days, which led to clearance of the mucocutaneous lesions and improvement in the tinnitus. A subsequent audiogram showed improvement in his hearing loss after 3 months.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for palmoplantar lesions of secondary syphilis includes palmoplantar psoriasis and pustulosis, palmoplantar eczema, keratoderma blennorrhagicum, tinea manuum, and pityriasis rosea. The presence of a peripheral rim of scale (Biett sign, Biett collarette) and pain caused by blunt pressure on these lesions (Buschke-Ollendorff sign) helps differentiate them from other conditions. Biett collarette may also be seen with lesions of porokeratosis and pityriasis rosea when they occur on the palms. However, porokeratosis generally causes scales that are rough and uneven, and pityriasis rosea produces multiple fine scales with an undefined direction.1 Palmo plantar lesions may have a configuration resembling erythema multiforme2 and rarely present as interdigital papules (condyloma lata) or erosions.3
Incidence rates of syphilis are known to be substantially higher in the HIV-positive population,4 and the secondary incubation period of syphilis is usually shortened in these patients. However, in our patient, manifestations of secondary syphilis were delayed by 9 months after exposure.
Incidence rates of otosyphilis in the HIV population are not well known. In a recent case series of 12 patients with otosyphilis, 8 (67%) were positive for HIV.5
Otosyphilis is often a presumptive diagnosis based on positive serology in patients with cochleovestibular symptoms with no other likely causes. It may present differently depending on the stage of syphilis. Sensorineural hearing loss (often bilateral and rapidly progressing) and tinnitus are the most common complaints in secondary syphilis. The presence of cerebrospinal fluid findings with otosyphilis ranges from 5.6% to 67%.5,6
The presentation of secondary syphilis is highly variable, including its dermatologic manifestations, earning it the name of the “great masquerader.” However, the presence of copper-colored patches and plaques on the palms and soles necessitates that syphilis be ruled out before considering other diagnoses.
It is imperative to ask any patient with syphilis about symptoms of ocular, otologic, and central nervous system involvement and to evaluate accordingly, thus saving the patient from considerable morbidity.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.