


Article Figures & Data
Figures
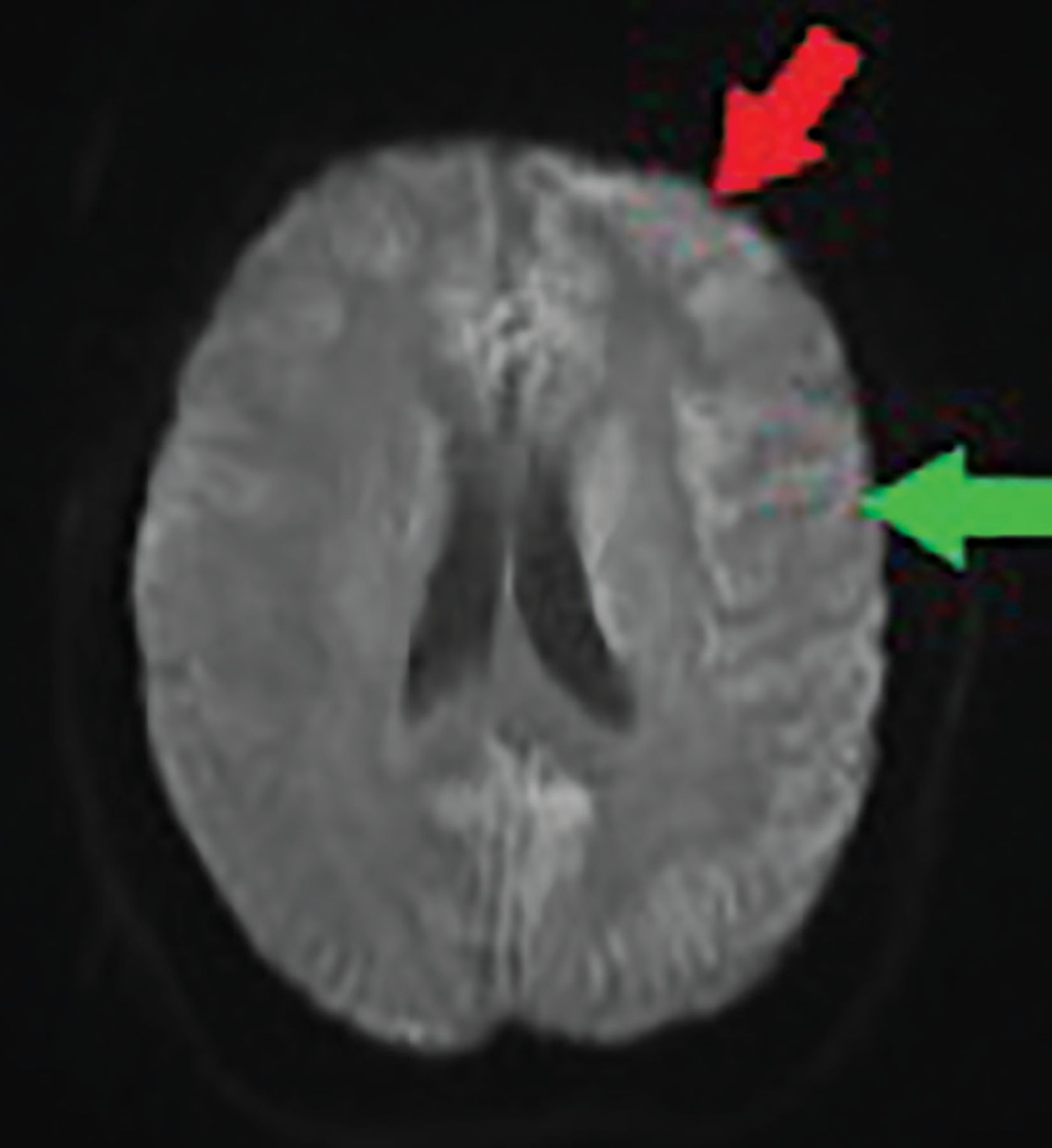
- Figure 1
Diffusion-weighted magnetic resonance imaging at admission shows cortical bifrontal (red arrow) and parietal (green arrow) diffusion (cortical ribboning), with greater intensity on the left. No thalamic hyperintensity was seen. Note that the quality of this image was affected by patient movement during the procedure, in spite of attempts to sedate her.
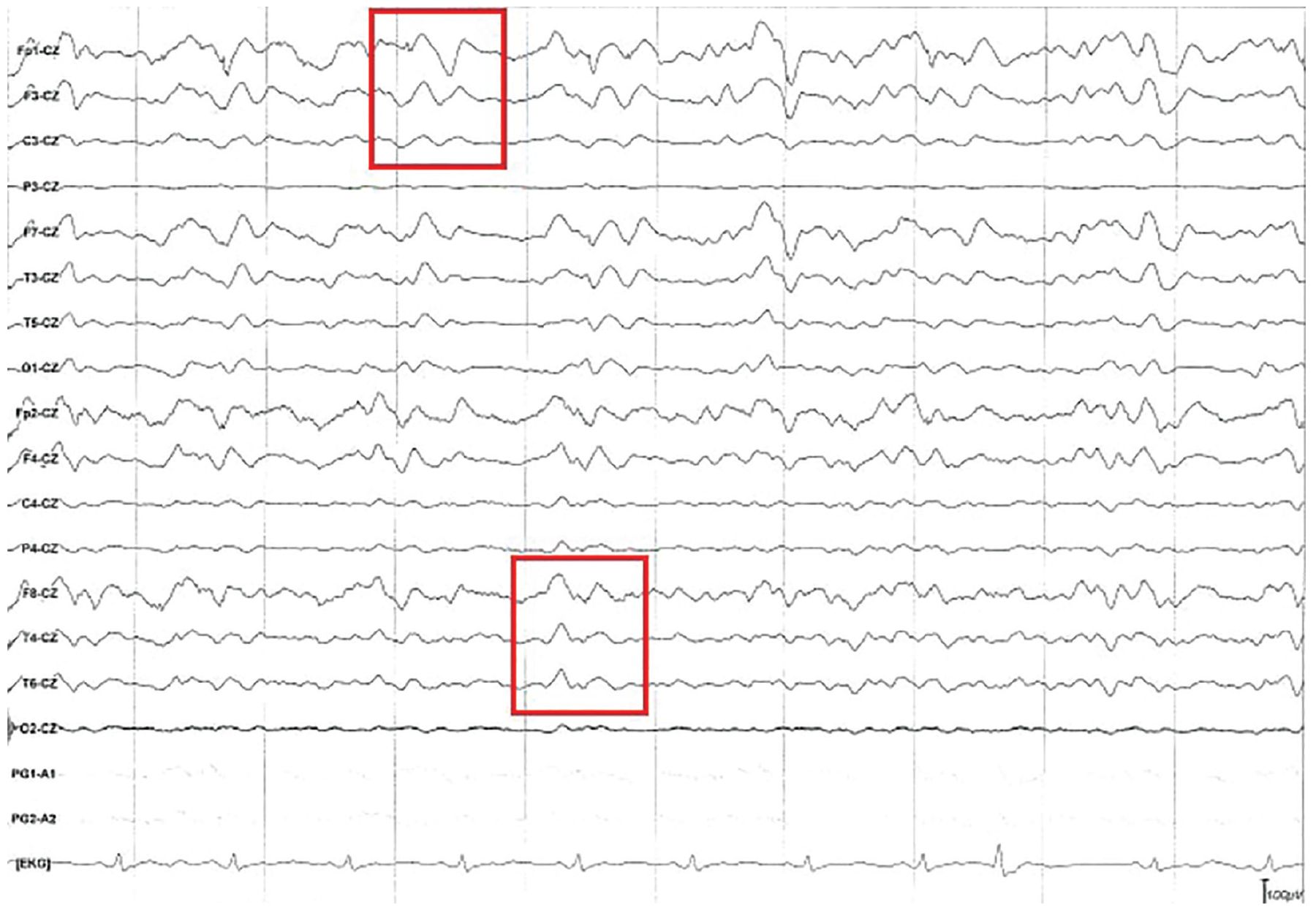
- Figure 2
Electroencephalography showed continuous triphasic waves (red boxes) and diffuse cortical slowing. Diffuse slowing is seen throughout the recording, as the background frequency consists mostly of theta waves (frequency 4–7 Hz) despite provoking maneuvers and the patient not being on sedating medications.
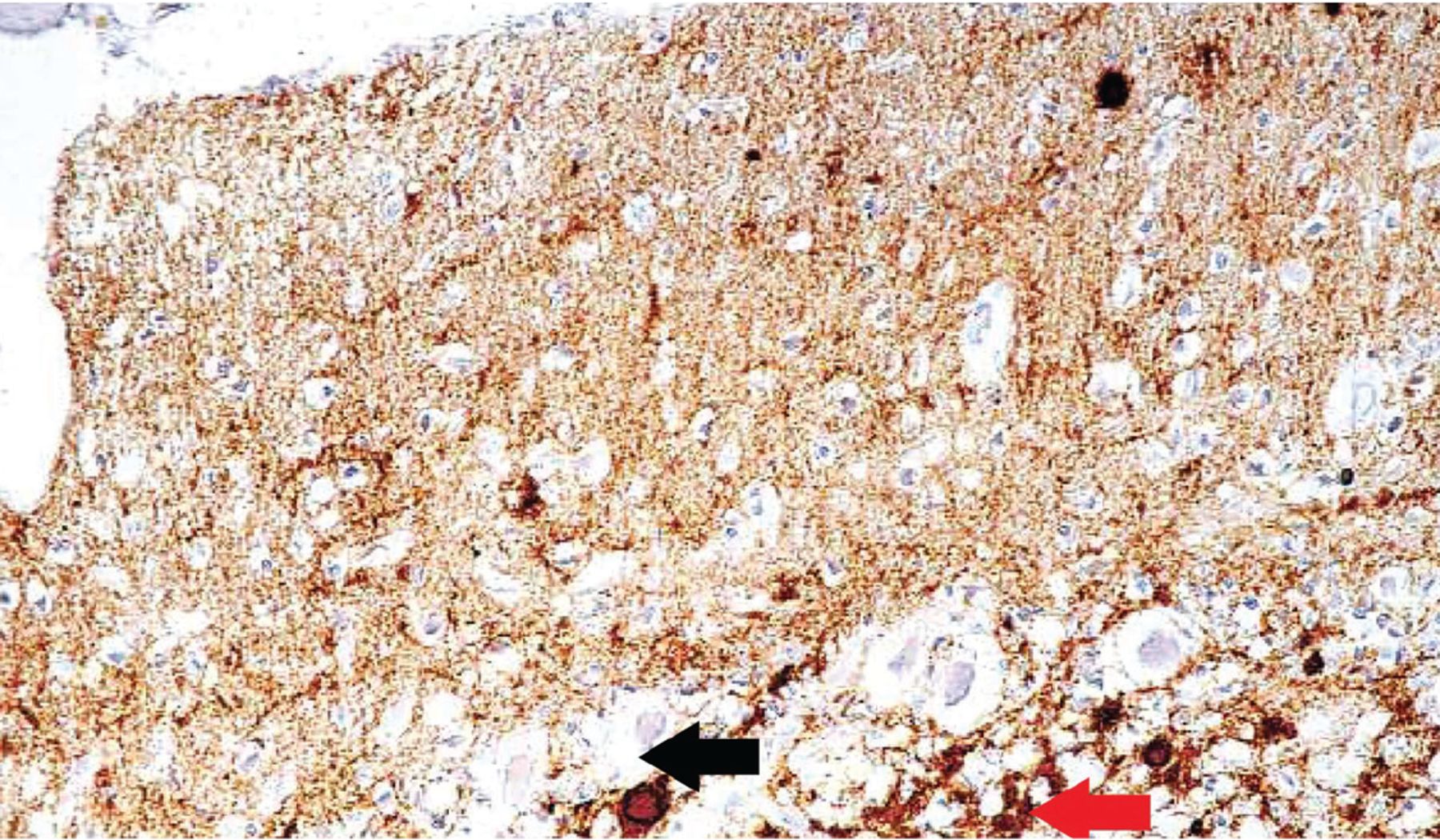
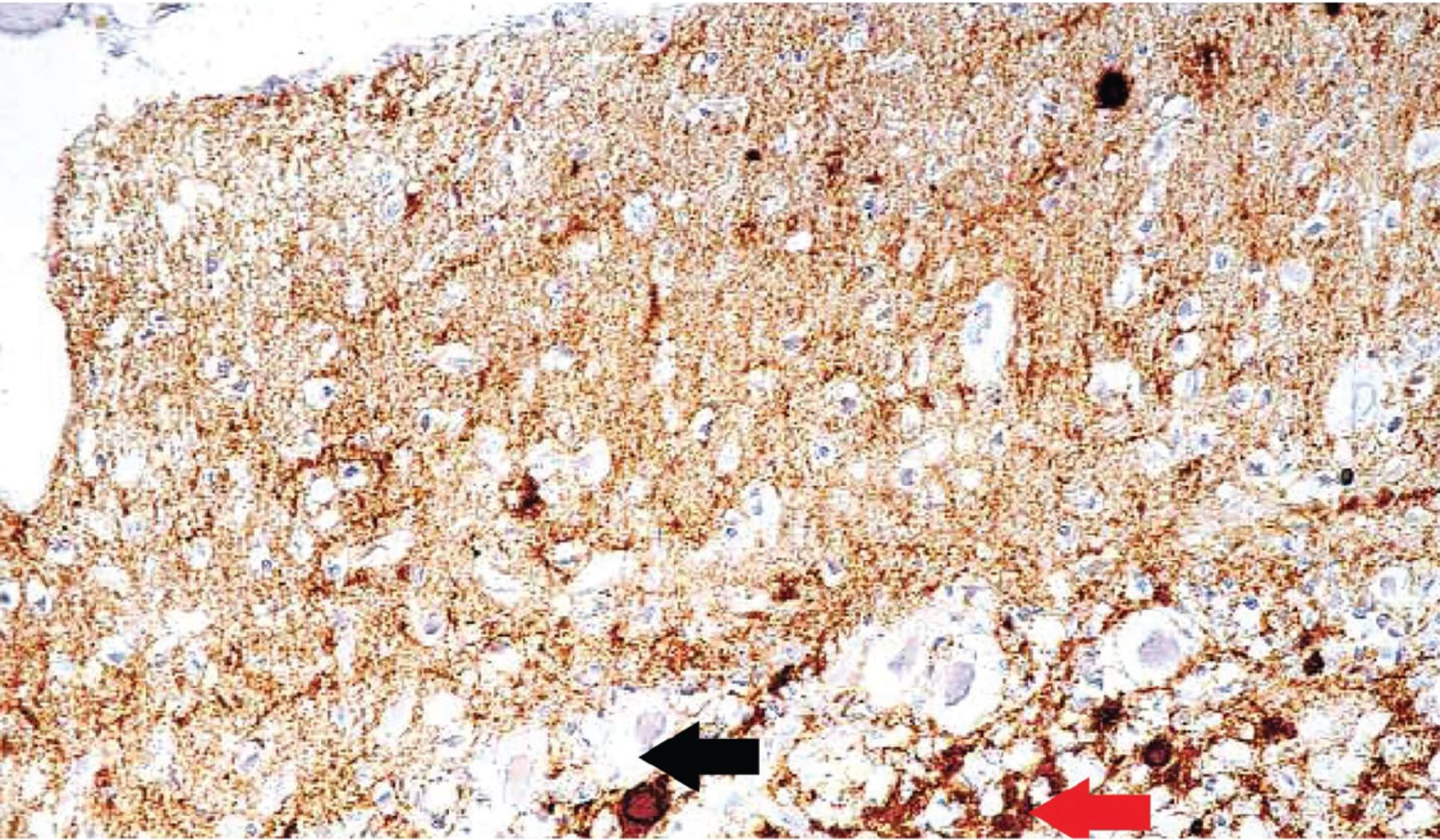
- Figure 3
Immunohistochemical staining shows fine prion protein deposits in the molecular layer, coarser deposits in the granular layer, and plaques in both layers of the cerebellum (magnification × 600). Fine deposits in the upper portion (molecular layer) of the image appear as numerous dark deposits. The red arrow points to coarse deposits in the granular layer, and the black arrow points to plaque.
From Kovács GG, Head MW, Hegyi I, et al. Immunohistochemistry for the prion protein: comparison of different monoclonal antibodies in human prion disease subtypes. Brain Pathol 2002; 12(1):1–11. doi:10.1111/j.1750-3639.2002.tb00417.x. Copyright John Wiley and Sons, Inc. Reprinted with permission.

Tables
Testing Sensitivity Specificity Diagnostic criteria Notes Magnetic resonance imaging DWI or FLAIR30 83% 83% At least 2 cortical regions affected (parietal–temporal–occipital) or both putamen and nucleus caudatum affected Retrospective evaluation of pathology-proven CJD DWI and FLAIR31 91% 95% 2005 UCSF MRI criteria for CJD31 Retrospective evaluation of clinically diagnosed prion disease, majority spontaneous CJD (83%); excellent interreader reliability (kappa 0.96) DWI and FLAIR32 96% 93% 2005 UCSF MRI criteria for CJD31 Retrospective evaluation of clinically diagnosed prion disease, majority spontaneous CJD (79%) DWI33 92% 94% High-intensity lesions in the striatum (caudate or putamen, or both), lesions in the thalamus including the pulvinar, and/or lesions along the cortical ribbon (cerebral or cerebellar) Retrospective evaluation of clinically diagnosed prion disease, majority spontaneous CJD (78%) Electroencephalography32 64% 91% 1996 Steinhoff criteria27 Retrospective evaluation of pathology-proven CJD Cerebrospinal fluid studies34 14-3-3 protein 83% 63% Positive test Retrospective analysis of 111 neuropathologically confirmed sCJD cases Total tau protein 91% 46% Positive test RT-QuIC 92% 99% Positive test CJD = Creutzfeldt-Jakob disease; DWI = diffusion-weighted imaging; FLAIR = fluid-attenuated inversion recovery; RT-QulC = real-time quaking-induced conversion; sCJD = sporadic Creutzfeldt-Jakob disease; UCSF = University of California, San Francisco
Neuropsychiatric disorder plus positive RT-QuIC in cerebrospinal fluid or other tissues
OR
All 3 of the following subcriteria:
Rapidly progressive dementia and at least 2 of these 4 clinical features:
Myoclonus
Visual or cerebellar disturbances
Pyramidal or extrapyramidal dysfunction
Akinetic mutism
A positive result on at least 1 of the following laboratory tests:
Typical electroencephalogram (periodic sharp-wave complexes) during an illness of any duration
Positive 14-3-3 protein cerebrospinal fluid assay in patient with a disease duration of less than 2 years
High signal in caudate and/or putamen on MRI, or in at least 2 cortical regions (temporal, parietal, occipital) on DWI or FLAIR
No routine investigation indicates an alternative diagnosis
CJD = Creutzfeldt-Jakob disease DWI = diffusion-weighted imaging; FLAIR = fluid-attenuated inversion recovery; MRI = magnetic resonance imaging; RT-QulC = real-time quaking-induced conversion.
From US Centers for Disease Control and Prevention, reference 41.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- DIFFERENTIAL DIAGNOSIS: DISEASES, CONDITIONS TO RULE OUT
- CASE CONTINUED
- AUTOANTIBODY ENCEPHALITIS: WHAT TO LOOK FOR
- CASE CONTINUED
- NEXT STEP: ADDITIONAL IMAGING
- CASE CONTINUED
- WHY TEST FOR PRION DISEASE?
- CASE CONTINUED
- EPIDEMIOLOGY OF PRION DISEASES
- PATHOLOGY DRIVES PRECAUTIONS
- TREATMENT AND PROGNOSIS
- TAKE-HOME MESSAGES
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.