


ABSTRACT
Estimating the risk of atherosclerotic cardiovascular disease (ASCVD) is a daily challenge for clinicians and is crucial to tailoring preventive medical care and guiding shared decision-making. New imaging modalities and novel biomarkers allow for more accurate assessment of patient risk and minimize the risk of over- or undertreating patients. Major cardiovascular medicine societies have incorporated new diagnostic modalities in their guidelines to aid clinical decision-making for primary and secondary prevention of ASCVD. This review presents commonly encountered cases relevant to estimating and reducing ASCVD risk based on available guidelines and expert opinion.
The coronary artery calcium score may be used in patients with borderline or intermediate risk of ASCVD to guide statin initiation.
Lipoprotein(a) is an important and often overlooked risk factor for ASCVD.
A therosclerotic cardiovascular disease (ASCVD) is the leading cause of morbidity and mortality worldwide.1 Statins have been the mainstay therapy in the primary prevention of ASCVD, while the role of aspirin in this patient population has been decreasing.2,3 However, the decision of starting either medication, particularly for primary prevention, can be challenging due to either the lack of benefit or the absence of robust data for certain age groups or patient subpopulations. With the availability of advanced imaging modalities and novel biomarkers, guidelines have amended the indications for primary and secondary prevention of ASCVD, incorporating new therapies to further reduce patient residual risk of ASCVD.2–4 In this case-based review, we present commonly encountered clinical cases that may pose clinical challenges for both internists and cardiologists in dealing with decisions on primary and secondary prevention of ASCVD.
CASE 1
A 58-year-old white male presented to the outpatient clinic for routine annual visit. On examination, his blood pressure was 146/88 mm Hg and his body mass index (BMI) was 29 kg/ m2. He confirmed being a current smoker. Lab results revealed hemoglobin A1c (HbA1c) of 8.9% (reference range 4%−5.6%), total cholesterol 147 mg/dL (reference range < 200 mg/dL), high-density lipoprotein cholesterol (HDL-C) 54 mg/dL (reference range > 40 mg/dL), low-density lipoprotein cholesterol (LDL-C) 92 mg/dL (reference range < 100 mg/dL), and spot urine albumin-to-creatinine ratio > 300 mg/g (reference range < 30 mg/g). He regularly takes lisinopril and hydrochlorothiazide. Concerned about his mother’s death from myocardial infarction at the age of 48, the patient is looking for risk-reduction strategies of future cardiovascular events. Other than emphasizing a healthy lifestyle and controlling blood pressure and diabetes, how would you further manage this patient?
Initiate simvastatin 40 mg
Initiate rosuvastatin 10 mg and aspirin 81 mg
Initiate atorvastatin 80 mg
Initiate rosuvastatin 40 mg and aspirin 81 mg
Answer: D
CASE 2
A 50-year-old African American female presented to the preventive cardiology clinic for an annual check-up with a history of rheumatoid arthritis and preeclampsia during her first pregnancy and her mother having passed away at the age of 45 from myocardial infarction. On examination, her blood pressure was 155/85 mm Hg and her BMI was 25 kg/m2. She exercises 4 times per week and does not use nicotine or alcohol. Her lipid profile revealed total cholesterol 200 mg/dL, HDL-C 33 mg/dL, and LDL-C 160 mg/dL. Moreover, HbA1c was 4.8% and high-sensitivity C-reactive protein (hs-CRP) was 4 mg/L (reference range < 3.0 mg/L). Other than controlling the patient’s hypertension, which of the following would be the best option to reduce risk of future ASCVD events?
Initiate atorvastatin 20 mg
Initiate atorvastatin 80 mg and aspirin 81 mg
Initiate atorvastatin 80 mg
Initiate atorvastatin 20 mg and aspirin 81 mg
Answer: C
RATIONALE
In case 1, the patient had a 10-year risk of ASCVD of 22.7% (high risk) that qualified him for high-intensity statin therapy (rosuvastatin 40 mg or atorvastatin 40–80 mg). In addition to his high ASCVD risk, the patient did not seem to be at elevated risk for bleeding. Therefore, it is reasonable to add low-dose aspirin after clinician-patient discussion about risks and benefits.
In case 2, the patient presented with a 10-year ASCVD risk of 8.4% (intermediate risk). However, the patient had a history of rheumatoid arthritis, preeclampsia, family history of premature heart disease, and elevated hs-CRP (> 2 mg/L). The pooled cohort equation may underestimate the 10-year ASCVD risk in patients with chronic inflammatory disorders such as those with human immunodeficiency virus (HIV) taking antiretroviral therapy, patients with rheumatoid arthritis or sarcoidosis. Therefore, it may be beneficial to consider other risk-enhancing factors in overall ASCVD risk assessment, especially because some factors may be targeted with specific therapies.2,3,5–7 While her 10-year ASCVD risk score suggested the initiation of moderate-intensity statins, the risk-enhancing factors highlighted above would favor a more aggressive approach with high-intensity statins, with atorvastatin 80 mg. The use of aspirin in this patient with intermediate ASCVD risk would likely yield greater net harm.
EVIDENCE
The role of statins in the prevention of ASCVD
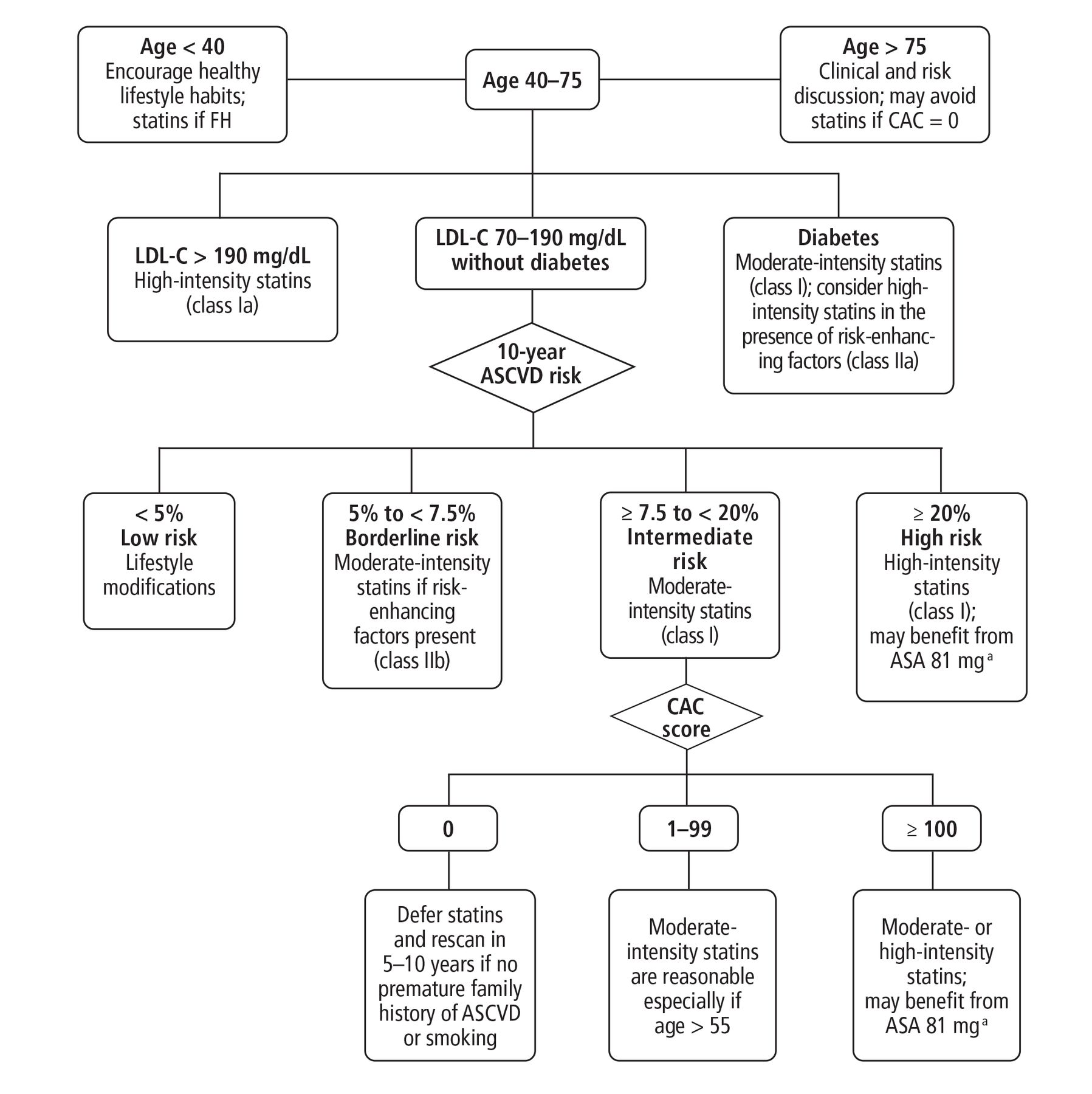
The role of statins in primary prevention of ASCVD among adults has been validated in several studies and strongly supported by major cardiovascular medicine societies.2,3,8–10 The American Heart Association (AHA) and American College of Cardiology (ACC) recommend statin therapy for primary prevention for patients if LDL-C levels exceed 190 mg/dL, if they have diabetes, or if they are 40 to 75 years of age with increased risk of ASCVD (≥ 7.5%) after clinician-patient discussion of the potential benefits and harms.2,3 Figure 1 summarizes the current evidence algorithm for using aspirin and statins for primary prevention of ASCVD.2,3,11 The role of statins in the elderly (> 75 years of age) is less certain, and thus their use must be tailored to every patient after discussing the risks and benefits.2 The latest ACC/AHA Blood Cholesterol and Primary Prevention of ASCVD guidelines state that statin therapy is reasonable in elderly patients who are expected to derive net clinical benefit from treatment.2,3 A meta-analysis from the Cholesterol Treatment Trialists’ Collaboration group12 among 14,483 adults and a more recent retrospective cohort study13 among 326,981 older US veterans (mean age 81) without ASCVD who were followed for approximately 6.8 years showed that initiation of statin therapy was significantly associated with reductions in major cardiac events in this population, including cardiovascular mortality (hazard ration [HR] = 0.80, 95% confidence interval [CI] 0.78−0.81), and all-cause mortality (HR = 0.75, 95% CI 0.74−0.76]).12,13 Importantly, potential side effects of statins are of concern in the elderly population mainly due to their more complicated health status and frailty. On the other hand, statins require about 4 to 5 years to show stroke-reducing benefits suggesting that patient life expectancy should also be considered in the overall decision-making process to direct statin therapy.2,3

Decision-making flowchart to guide strategies for reducing the risk of atherosclerotic cardiovascular disease.
aAvoid aspirin use in patients with a high risk of bleeding.
ASA = acetylsalicylic acid; ASCVD = atherosclerotic cardiovascular disease; CAC = coronary artery calcium; FH = familial hypercholesterolemia; LDL-C = low-density lipoprotein cholesterol Adapted from Grundy et al, reference 2.
The estimation of the individual’s 10-year ASCVD risk score using the pooled cohort equation remains the mainstay for primary prevention.2,3 The ASCVD calculator (https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/) is available for free online and offers a clinical decision tool. Furthermore, the latest ACC/AHA guidelines on the primary prevention of cardiovascular disease highlighted several risk-enhancing factors to guide treatment decisions2,3:
Family history of premature ASCVD
Persistently elevated LDL-C ≥ 160 mg/dL
Chronic kidney disease
Metabolic syndrome
Preeclampsia and premature menopause
Chronic inflammatory diseases (eg, rheumatoid arthritis, psoriasis, HIV)
High-risk race or ethnicity (eg, South Asian ancestry)
Persistently elevated triglycerides ≥ 175 mg/dL.
The following are measurable risk factors:
hs-CRP ≥ 2.0 mg/L
Lipoprotein(a) (Lp[a]) levels ≥ 50 mg/dL or 125 nmol/L
Apolipoprotein B ≥ 130 mg/dL
Ankle-brachial index < 0.9.
In adults at intermediate risk (7.5% to 20%), moderate-intensity statins are indicated to decrease LDL-C levels by 30% or more. However, in those with high ASCVD risk (> 20%), high-intensity statins are recommended to reduce LDL-C levels more than 50%.2
Aspirin and primary prevention of ASCVD
The role of aspirin in secondary prevention is well established; however, its role in primary prevention has been debatable and recently studied in multiple large randomized clinical trials targeting different patient populations.14 As such, the latest guidelines on cardiovascular disease prevention from the European Society of Cardiology do not recommend the use of aspirin in primary prevention (low-to-moderate risk patients), while the American Diabetes Association recommends that aspirin therapy (75–162 mg/ day)15 may be considered for primary prevention if the patient is at increased risk of cardiovascular disease.16,17
Three recent large-scale clinical trials18–20 provided concrete evidence on the role of aspirin in primary prevention. The ARRIVE (Aspirin to Reduce Risk of Initial Vascular Events) trial,18 a prospective, randomized, double-blinded trial, included 12,546 patients without diabetes at moderate risk of ASCVD. Aspirin 100 mg/day did not reduce the primary outcome of composite all-cause or cardiovascular mortality. Instead, it significantly increased gastrointestinal bleeding (HR 2.11, P = .0007). The ASCEND trial (A Study of Cardiovascular Events in Diabetes)19 investigated outcomes with aspirin 100 mg/day in 15,480 patients with diabetes without established cardiovascular disease and did not show a reduction in all-cause or cardiovascular deaths. Although, major bleeding events were increased significantly with an absolute risk increase of 0.9% (number needed to harm = 111), the number needed to treat (NNT = 91) to prevent an ASCVD event remained lower based on an absolute risk reduction of 1.1%. Further, in patients age 70 or older, the use of aspirin for primary prevention was associated with higher all-cause mortality in the ASPREE trial (Aspirin in Reducing Events in the Elderly),20 which enrolled 19,114 patients assigned to receive 100 mg of enteric-coated aspirin or placebo (HR = 1.14, 95% CI 1.01−1.29).20
In light of the accumulating evidence on the limited role of aspirin in primary prevention for ASCVD and potential harm associated with it in the trials highlighted above as well as prior multiple meta-analyses, the most recent ACC/AHA guidelines recommend low-dose aspirin (75–100 mg/day) for the primary prevention of ASCVD in select adults ages 40 to 70 who have elevated ASCVD risk but are not at increased bleeding risk (class of evidence IIb, level of evidence A).2,3 Factors associated with increased risk of bleeding include history of gastrointestinal bleeding, chronic predisposing conditions such as coagulopathy, chronic kidney disease, chronic inflammatory conditions with use of nonsteroidal anti-inflammatory medications, and use of anticoagulation.
Alternatively, the role of coronary artery calcium (CAC) scores to direct aspirin initiation for primary prevention of ASCVD has been illustrated in some observational studies.21,22 In one analysis from the Multiethnic Study of Atherosclerosis cohort,21 patients with CAC score of zero Agatston units are less likely to benefit from aspirin therapy even with family history of premature cardiovascular disease. In another analysis from the Multiethnic Study of Atherosclerosis trial,22 CAC scores were more likely to identify subgroups that would benefit from aspirin therapy in patients with high ASCVD risk scores compared with pooled cohort equations. According to this analysis, only patients with a CAC score ≥ 100 Agatston units would gain net clinical benefit from aspirin for primary prevention, while the use of aspirin in patients with a CAC score < 100 Agatston units would probably yield greater net harm. However, in the absence of robust data and the concomitant risk of radiation exposure, the use of CAC scores to direct aspirin therapy in intermediate risk patients is still under investigation.
CASE 3
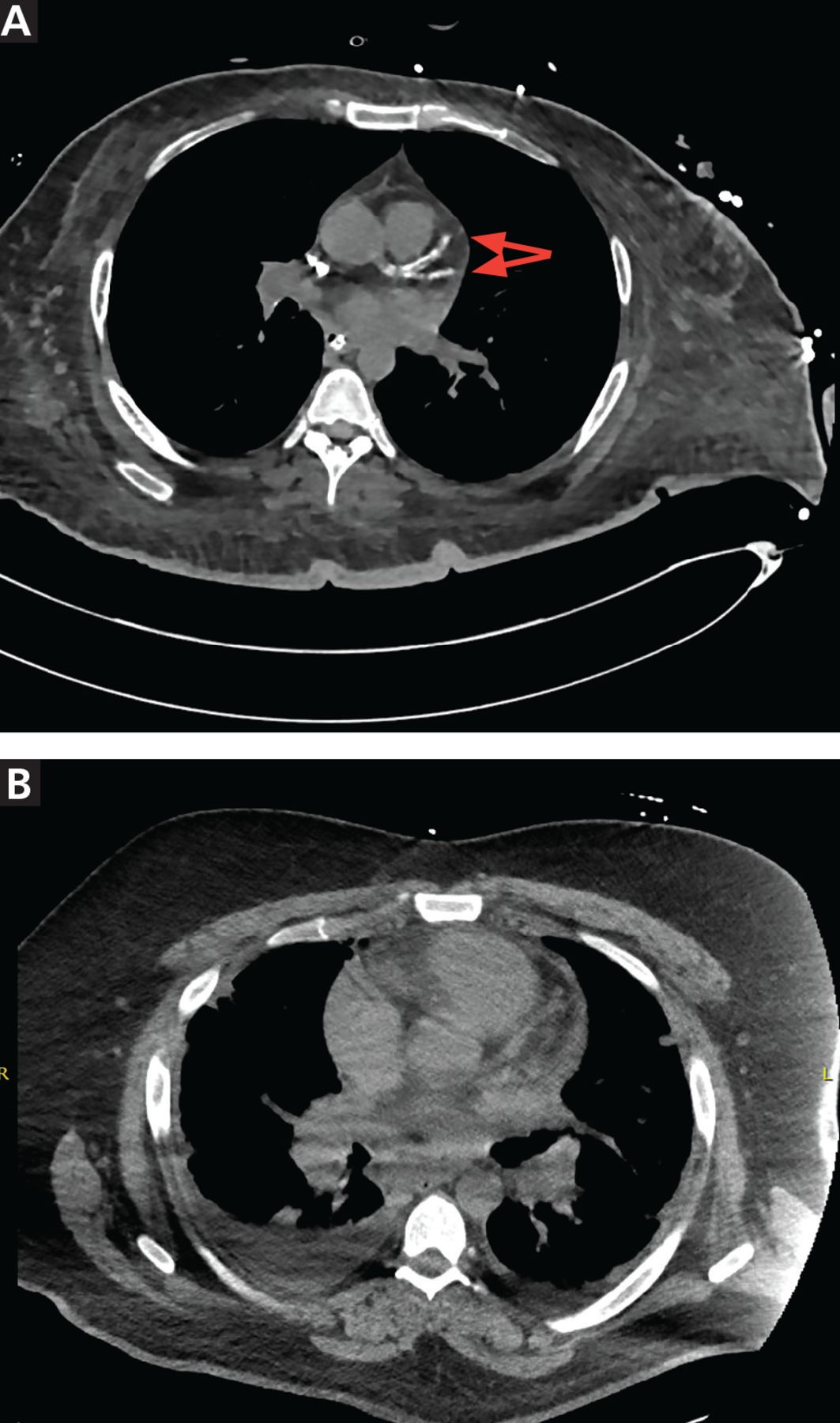
A 44-year-old African American male with a history of well-controlled hypertension and HIV on antiretroviral therapy, presented to the clinic for an annual physical examination and to establish care. He had no history of family with premature heart diseases. On examination, his blood pressure was 125/79 mm Hg and BMI was 35 kg/m2. The rest of the physical examination was non-revealing. Blood tests showed LDL-C 123 mg/dL, HDL-C 49 mg/dL, total cholesterol 223 mg/dL, triglycerides 255 mg/dL (reference range < 160 mg/dL), and serum creatinine 0.9 mg/ dL (reference range 0.6 to 1.3 mg/dL). He is a former smoker (quit 20 years ago) with a sedentary lifestyle. Review of outside records revealed cardiac computed tomography done within the year with a CAC score of zero Agatston units (Figure 2). Which of the following would you recommend for this patient?
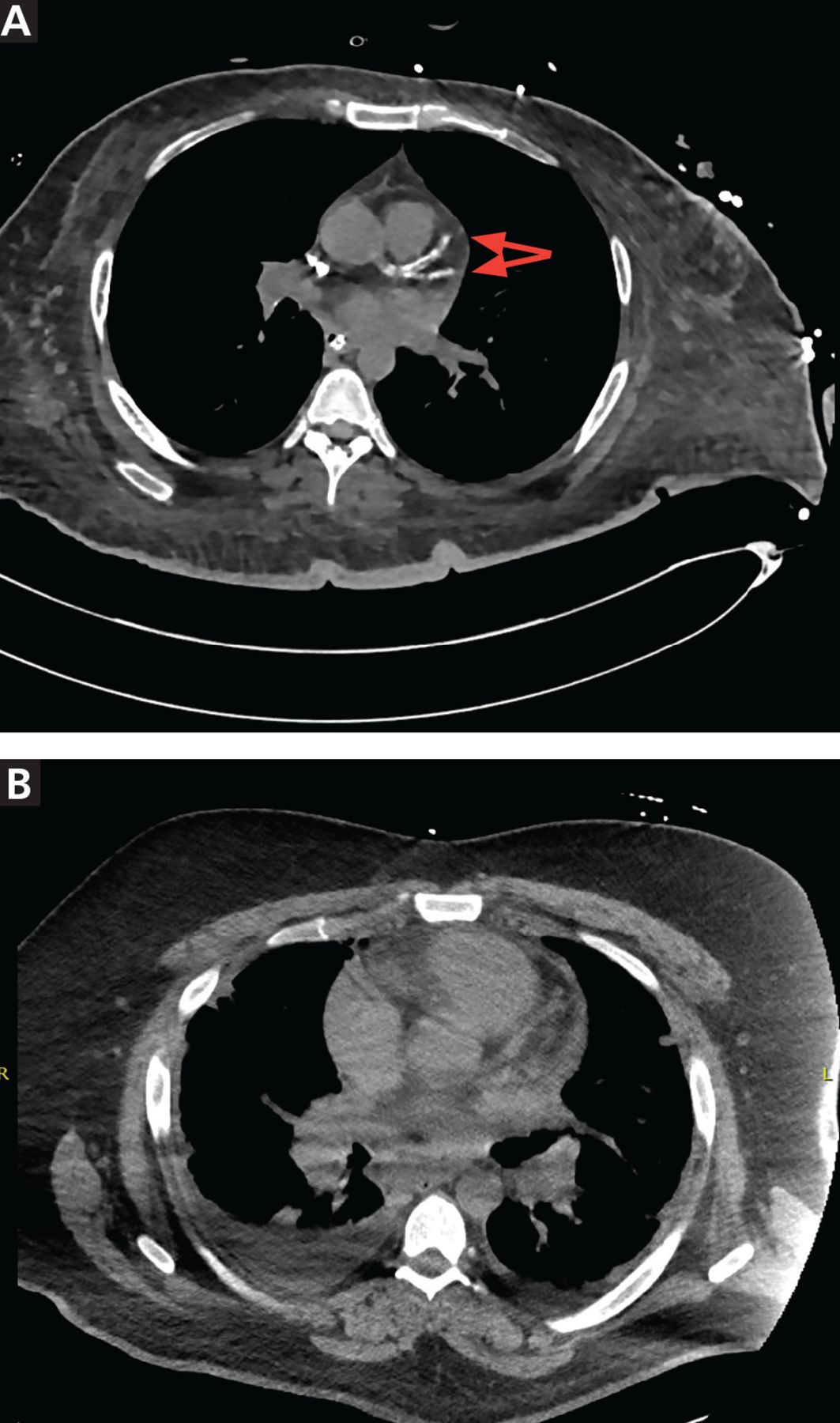
Cardiac computed tomography showing (A) significant coronary calcification (arrows) and a high coronary artery calcium score, and (B) a coronary artery calcium score of zero Agatston units.
Initiate atorvastatin 20 mg
Initiate aspirin 81 mg
Initiate atorvastatin 20 mg and aspirin 81 mg
Measure serum Lp(a)
Encourage healthy lifestyle changes for weight loss and smoking cessation
D and E
Answer: F
RATIONALE
The patient in case 3 has a 10-year ASCVD risk score of 6.4% (borderline). In the absence of coronary calcification with a CAC score of zero Agatston units, it is reasonable to withhold statin therapy and reassess in 5 to 10 years (class of evidence IIa; level of evidence B).4 Further, measurement of Lp(a) is a reasonable once-in-a-lifetime test, is an affordable screening tool, can establish a reference value, and can qualify patients for risk-reducing therapies. Importantly, statins interact with several antiretroviral agents, particularly protease inhibitors, and can increase the risk of toxicity associated with statins, including myopathy and rhabdomyolysis.2
EVIDENCE
The role of coronary artery calcium scoring in the primary prevention of ASCVD
The latest AHA/ACC cholesterol management guideline sheds light on the role of CAC testing to further stratify patients with borderline to intermediate ASCVD risk.2,3 While the pooled cohort equation remains the cornerstone to estimate ASCVD risk, it can overestimate or underestimate risk in some subpopulations.23 Hence, it is reasonable to consider individual risk factors that may refine patient risk and subsequently individualize treatment strategy. However, if risk assessment is still uncertain after accounting for risk-enhancing factors in patients with borderline or intermediate risk or if the patient is still reluctant to start treatment, obtaining a CAC score is reasonable (class IIa).2,3,11 The following include scenarios where obtaining a CAC score and knowing the score is zero would support clinical decision-making:2,3
Patients reluctant to initiate statin who wish to understand their potential risk and benefit more precisely
Patients who are not adherent to statin therapy due to side effects but are willing to reinitiate statins for risk reduction
Older patients (men ages 55–80, women ages 60–80) with low burden of cardiovascular risk factors who question the benefit from statins
Middle-aged adults (ages 40–55) with a 10-year risk of ASCVD 5% to < 7.5%, in the absence of high-risk conditions such as cigarette smoking, family history of premature ASCVD, or diabetes mellitus.
If risk is still uncertain after accounting for risk-enhancing factors in patients with borderline or intermediate risk, obtaining a CAC score is reasonable
The measurement of subclinical atherosclerosis by CAC is generally preferred over serum biomarkers for the prediction of future ASCVD.24,25 Data from the CAC Consortium showed that CAC is the most reliable predictor for atherosclerotic cardiovascular diseases and may be an integral component of the risk stratification especially in ethnic minorities or certain age groups where the pooled cohort equation tends to either underestimate or overestimate risk.26 CAC may also play a role in reducing cardiovascular NNT with statins.27 For example, one cohort study done among 13,644 patients from the Walter Reed Army Medical Center showed that statin therapy was associated with reduced risk of major adverse cardiovascular events only in patients with non-zero CAC scores.27 Interestingly, the NNT with statins in patients with CAC scores of zero to prevent major adverse cardiovascular events over median follow-up of 9.4 years was 3,571, which decreases to 100 in those with CAC scores between 1 and 100 Agatston units and 12 in those with CAC ≥ 101 Agatston units.27
Thus, a zero CAC score may be used to defer statin initiation in adults ages 40 to 75 without diabetes and with an LDL-C 70 to 189 mg/dL if there are no additional risk factors such as smoking or significant family history of premature ASCVD, and if the patient can be reassessed in 5 to 10 years (class of evidence IIa; level of evidence B).4 It is important to note that the vast majority of data regarding CAC scores to guide primary prevention of ASCVD is derived from observational studies, and physicians should be aware of risks associated with exposing patients to radiation with unclear long-term side effects associated with such exposure. Of note, the radiation exposure (mean 1 mSv) required to obtain a CAC score is comparable to that of mammogram screening.28 Therefore, clinician-patient discussion is highly encouraged when considering CAC measurements for further risk stratification.2
The role of lipoprotein(a) in cardiovascular disease prevention
The role of Lp(a) in the pathogenesis of ASCVD is well established.29 Promising results from recent early-stage clinical trials using targeted therapy for Lp(a) have shown substantial reductions from baseline levels.30 Yet, there are no clear thresholds to define high Lp(a) levels mainly due to heterogeneity in approaches to measure Lp(a) and prevalence among different patient populations.31 For example, Black individuals of African descent and South Asian populations have higher median Lp(a) levels than White or East Asian individuals.32 Moreover, around 70% to ≥ 90% heterogeneity of Lp(a) levels are genetically determined with an autosomal codominant inheritance pattern.31 Therefore, a single measurement could be sufficient to estimate patient ASCVD risk more accurately and allow for initiation of screening of family members due to the inheritance pattern and significant association with ASCVD burden. Hence, it is reasonable to measure Lp(a) in patients with poorly controlled LDL-C, including those already on high-intensity statins and ezetimibe along with patients with a strong family history of premature ASCVD.31 Yet it is important to note that some intraindividual temporal variability has been documented. Thus, obtaining the mean of two Lp(a) measurements at different times may be more clinically beneficial in refining risk prediction. Further studies are warranted to elucidate standard protocol for Lp(a) measurement.31
The latest ACC/AHA 2018 Blood Cholesterol guidelines stated that Lp(a) ≥ 50 mg/dL or 125 nmol/L (it is preferable to use an assay that reports Lp[a] levels in nmol/L) is considered a risk-enhancing factor with increasing significance at higher levels.2 Remarkably, the National Heart Lung and Blood Institute reported (2018) that an estimated 1.4 billion people globally have Lp(a) levels ≥ 50 mg/dL, with a prevalence ranging from 10% to 30% and possibly higher in patients with established ASCVD, calcific aortic valve disease, or chronic kidney disease,33 making Lp(a) a promising biomarker to further risk-stratify patients.34 In fact, measuring serum Lp(a) is of clinical significance as it has been shown to reclassify about 40% of individuals into either lower or higher risk groups.35 For instance, in the AIM-HIGH (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglyceride and Impact on Global Health Outcomes) trial, patients with controlled LDL-C had 89% higher risk of ASCVD with Lp(a) > 50 mg/dL compared with those with optimal levels.36 In a meta-analysis of 126,634 participants from 36 prospective studies, elevated Lp(a) was associated with a logarithmic increase in myocardial infarction and cardiovascular death (risk ratio 1.13, 95% CI 1.09−1.18).29 For example, patients had a risk ratio of coronary heart disease adjusted for age and sex of 1.16 per 3.5-fold elevation in Lp(a).29
To date, there are no US Food and Drug Administration-approved therapies that directly target elevated Lp(a); however, novel agents are in late stage clinical trials (National Clinical Trial [NCT]04023552). Nevertheless, the effect of currently available lipid-lowering agents on Lp(a) is modest and clinically not significant.31,37 For instance, in a systematic review and meta-analysis38 comparing ezetimibe to placebo in patients with primary hypercholesterolemia, there were minimal to no changes in Lp(a) levels. While proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have been shown to reduce Lp(a) levels by around 20% to 30%,39 this reduction is probably insufficient to reach targeted Lp(a) concentrations (< 50 mg/dL) in many patients.37 On the other hand, lipid apheresis has been shown to decrease Lp(a) by 50% to 75%. However, this procedure is expensive and needs to be performed every 1 to 2 weeks.37 Recently, ligand-conjugated antisense oligonucleotides have shown promising efficacy and safety in reducing Lp(a) in phase I/II clinical trials. Antisense oligonucleotides are short, single-stranded oligonucleotides that target mRNA of Lp(a) and degrade it by activating an enzyme called RNase H1 (ribonuclease H1). Pel-acarsen, formerly known as AKCEA-APO-(a)LRx, is one example of an antisense oligonucleotide that was shown to reduce Lp(a) by up to 92% in phase II clinical trials with excellent safety profiles.30,40 The HORIZON trial (Assessing the Impact of Lipoprotein [a] Lowering With Pelacarsen [TQJ230] on Major Cardiovascular Events in Patients With CVD)41 is a phase III, double blinded, placebo-controlled ongoing clinical trial investigating the effect of pelacarsen on cardiovascular outcomes in patients with established ASCVD. It has currently enrolled nearly 4,000 participants globally (more than 50% enrollment target) (NCT04023552).41
CASE 4
A 52-year-old African American female with a history of hypertension, diabetes, chronic kidney disease stage IV, coronary artery bypass graft 5 years ago, and a non-ST-segment elevation myocardial infarction 2 months ago, presented to the clinic for a follow-up visit. She was concerned about her cardiovascular risk after her 45-year-old brother suffered a massive myocardial infarction a few weeks prior and unfortunately passed away. Her medications included aspirin 81 mg, atorvastatin 80 mg, amlodipine 10 mg, and a multivitamin. On physical examination, her blood pressure was 137/74 mm Hg. Cardiac auscultation revealed a regular rhythm, no murmurs. Her ankle-brachial index was 0.60 (reference range 1−1.4) and lipid panel was as follows: LDL-C (92 mg/dL), HDL-C (49 mg/dL), and triglycerides (220 mg/dL). How would you further reduce this patient’s risk of future cardiovascular events?
Add ezetimibe therapy
Add a PCSK9 inhibitor
Add a PCSK9 inhibitor and ezetimibe
Continue current management
Answer: A
RATIONALE
In case 4, the patient has established ASCVD. Thus it is recommended to aggressively control her lipid profile to reduce her risk of future cardiovascular events. While she is on maximally tolerated statin therapy, her LDL-C is still above 70 mg/dL. Hence, the next reasonable step would be to add ezetimibe 10 mg/day. After 6 to 8 weeks, the patient would be re-evaluated for treatment efficacy. When the targeted LDL-C goal of < 70 mg/dL is not reached, the addition of a PCSK9 inhibitor is indicated. Obtaining a CAC score in such cases would not add valuable clinical information or alter treatment plans.
EVIDENCE
Beyond statins
Statins remain the foundation of LDL-C reduction in secondary prevention. However, in patients with established cardiovascular disease, maximally tolerated doses of statins are not sufficient to reach the targeted goal of < 70 mg/dL or at least 50% reduction in serum LDL-C from baseline. Hence, in such patients, especially in patients with a history of multiple ASCVD events who are at high risk of future disease, the use of non-statin medications is indicated.2 The first option to be considered as an adjunctive therapy is ezetimibe. Ezetimibe inhibits the uptake of cholesterol by interacting with the Niemann-Pick C1-like protein. Consequently, less cholesterol will be delivered to the liver, upregulating hepatocytic LDL-C receptors and leading to a decrease in serum LDL-C. Ezetimibe monotherapy decreases LDL-C by 18%; however, this percent reduction increases up to 27% when combined with a high-intensity statin regimen.42 Results from the IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International) trial favor the addition of ezetimibe to high-intensity statins if patients do not reach the LDL-C target with statin monotherapy.43 The most important finding from this trial is that lower LDL-C levels achieved in the sim-vastatin plus ezetimibe group translated into further reduction in major adverse cardiovascular events that were more prominent in patients with diabetes as well as those over age 75.43 Thus, patients at highest ASCVD risk derive the greatest benefit from LDL-C-lowering therapies.
Furthermore, if LDL-C remains above 70 mg/dL despite the use of dual lipid-lowering therapy, it is recommended to start PCSK9 inhibitors.2,4 To date, there are two US Food and Drug Administration-approved PCSK9 inhibitors, alirocumab and evolocumab. The approval was based on two major randomized controlled trials that evaluated efficacy and safety of PCSK9 inhibitors: the FOURIER and the ODYSSEY trials. In the FOURIER (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk) trial,44 patients had a baseline LDL-C ≥ 70 mg/dL or non-HDL-C ≥ 100 mg/dL. At follow-up (median, 2.2 years), evolocumab significantly reduced composite ASCVD (15% relative risk reduction). These results were replicated in the ODYSSEY (Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab) trial45 that investigated efficacy and safety of alirocumab in secondary prevention of patients on maximally tolerated statins. Although both trials did not reveal major adverse effects (< 3 years), the absence of longitudinal data raises concern over long-term safety profiles of these agents. While no trials to date have investigated whether the addition of ezetimibe or PCSK9 inhibitors to maximally tolerated statins is better, the use of ezetimibe as a second-line treatment before PCSK9 inhibitors is reasonable.4 First, ezetimibe is less costly and is now available in generic forms. Second, the long-term safety profile of this drug is well established. Finally, the combination of ezetimibe and high-intensity statins would be enough to reach LDL-C reduction target in the majority of patients.
TAKE-HOME POINTS
In patients with low or moderate 10-year ASCVD risk and low-density lipoprotein cholesterol (70–189 mg/dL), an assessment of potential risk-enhancing factors may be useful to clinicians in risk-stratifying patients and further directing medical therapy.
The CAC score may be used for patients with borderline or intermediate risk of ASCVD to guide statin initiation.
Lp(a) is an important risk factor for ASCVD with promising therapies in late-stage clinical trials.
The addition of ezetimibe or a PCSK9 inhibitor or both is proven to further reduce the risk of ASCVD when target LDL-C cannot be achieved with high-intensity statin monotherapy.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Footnotes
Dr. Nissen reports that the Cleveland Clinic Center for Clinical Research has received funding to perform clinical trials from Abbvie, AstraZeneca, Amgen, Eli Lilly, Esperion, Medtronic, MyoKardia, Novartis, Pfizer, and Silence Therapeutics. Dr. Nissen is involved in these clinical trials but receives no personal remuneration for his participation. Dr. Nissen consults for many pharmaceutical companies but requires them to donate all honoraria or consulting fees directly to charity so that he receives neither income nor a tax deduction.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.