


Article Figures & Data
Figures
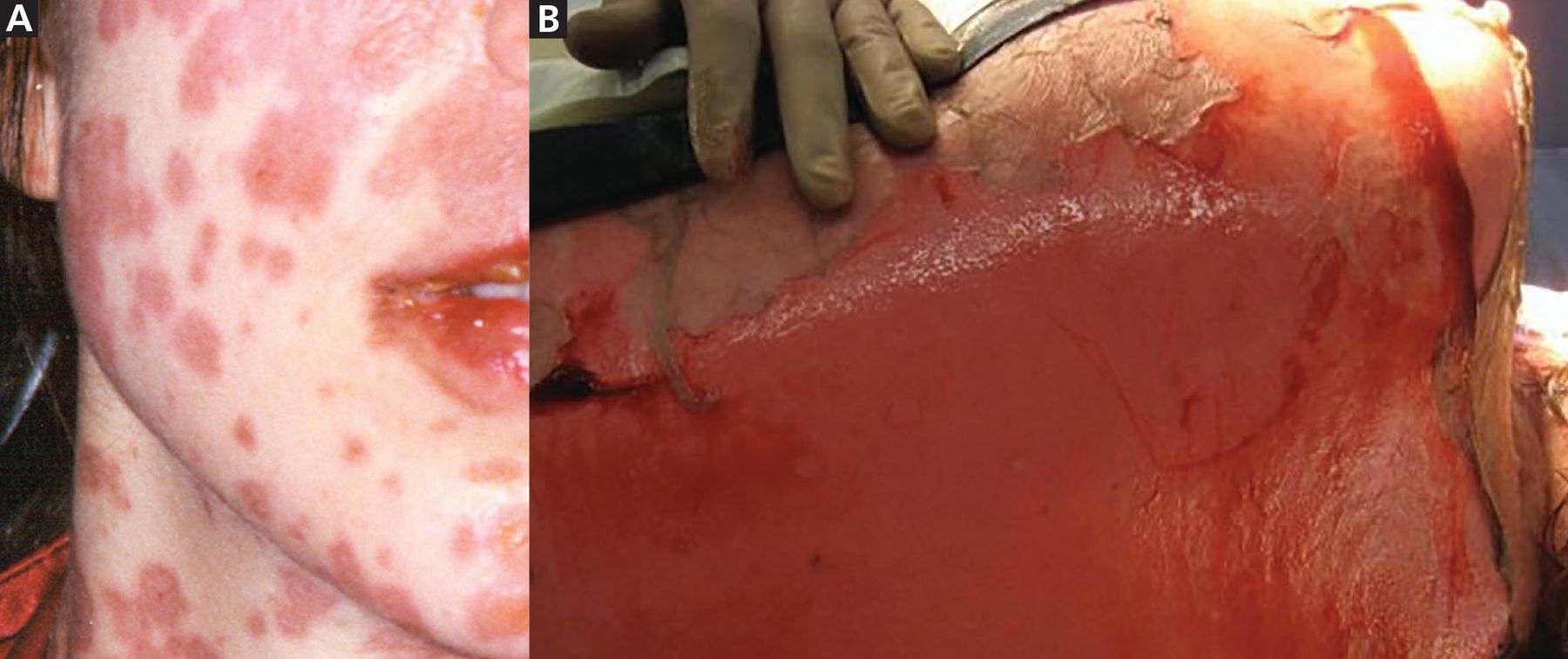
- Figure 1
(A) Macules and target-like lesions with erythema and dark necrotic centers in Stevens-Johnson syndrome. (B) Positive Nikolsky sign with epidermal shearing in Stevens-Johnson syndrome.
- Figure 2
(A) A maculopapular rash in a drug reaction with eosinophilia and systemic symptoms. (B) Lesions may also present as plaques, blisters, or target-like lesions.
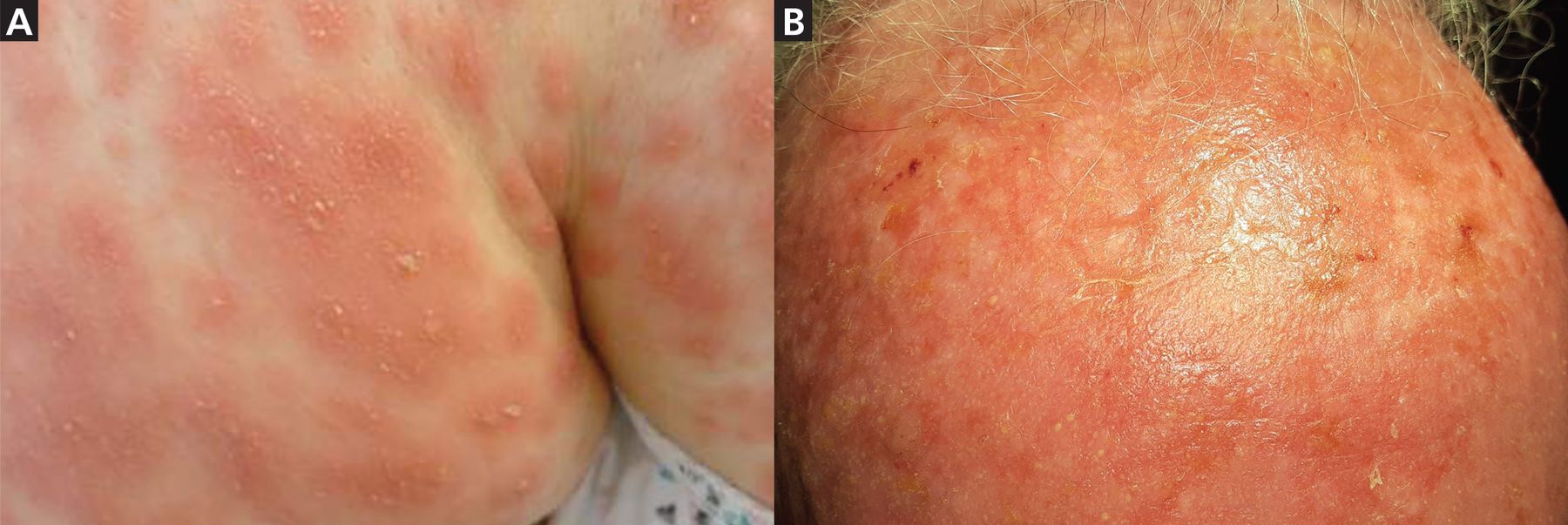
- Figure 3
(A) Pustules and diffuse edematous erythema in a patient with acute generalized exanthematous pustulosis affecting intertriginous folds and, (B) a patient’s forehead.
- Figure 4
Rash associated with drug-induced vasculitis. Bilateral presentation on dependent areas of the body is common.




Tables
Disease Onset Skin findings Hallmarks Drug triggers Diagnosisb SJS/TEN 1–3 weeks Red/purple macules progressing to vesicles, erosions, and ulcerations Mucous membrane involvement; Nikolsky sign Allopurinol, antibiotics (particularly sulfonamide), antiepileptics, NSAIDs SCORTEN DRESS 2–6 weeks Generalized maculopapular erythematous rash Facial edema and redness, eosinophilia, elevated transaminases Allopurinol, antibiotics, antiepileptics, antiretrovirals, isoniazid, NSAIDs RegiSCAR AGEP 48 hours Generalized maculopapular erythematous rash with pinpoint pustules Face, trunk, and intertriginous area; tiny pustules often difficult to see Antibiotics, antimycotics, diltiazem, hydroxychloroquine EuroSCAR; consider dermatoscopy Drug-induced vasculitis 1–3 weeks Palpable purpura Dependent areas, reverse koebnerization Allopurinol, amiodarone, antibiotics, beta-blockers, diuretics, metformin, NSAIDs, SSRIs Evaluate for alternative causes of systemic vasculitis ↵a Treatment starts with immediate identification and cessation of the offending drug.
↵b Consider skin biopsy to further support diagnosis for all these rashes.
AGEP = acute generalized exanthematous pustulosis; DRESS = drug reaction with eosinophilia and systemic symptoms; EuroSCAR = European Study of Severe Cutaneous Adverse Reactions; NSAIDs = nonsteroidal anti-inflammatory drugs; RegiSCAR = Registry of Severe Cutaneous Adverse Reactions; SCORTEN = Severity-of-Illness Score for Toxic Epidermal Necrolysis; SJS/TEN = Stevens-Johnson syndrome/toxic epidermal necrolysis; SSRIs = selective serotonin reuptake inhibitors
SCORTEN parameter Point Age ≥ 40 1 Malignancy 1 Heart rate ≥ 120 beats per minute 1 Initial surface of epidermal detachment > 10% 1 Serum urea > 10 mmol/L 1 Serum glucose > 14 mmol/L 1 Bicarbonate ≤ 20 mmol/L 1 Total score Predicted mortality risk (%) 0–1 3.2 2 12.1 3 35.8 4 58.3 > 5 90 Adapted from information in references 4 and 10.
- TABLE 3
Registry of Severe Cutaneous Adverse Reactions diagnostic criteria for drug reaction with eosinophilia and systemic symptoms
Criteriaa Scoreb No Yes Unknown 1) Acute skin eruption a) More than 50% body surface area affected 0 +1 0 b) Rash characteristic of DRESS -1 +1 0 c) Biopsy suggesting DRESS -1 0 0 2) Fever > 38.5°C -1 0 -1 3) Lymphadenopathy (> 1 site, > 1 cm) 0 +1 0 4) Internal organ involvementc 0 +1 0 5) Eosinophilia a) Eosinophils 700-1,499, or 10%-19.9%
if leukocytes < 4.0 × 109 L+1 b) Eosinophils > 1,500 or > 20%
if leukocytes < 4.0 × 109 L+2 6) Atypical lymphocytes 0 +1 0 7) Thrombocytopenia Additional parameters Resolution in > 15 days -1 0 -1 Exclusion of: antinuclear antibodies, blood culture, serology for hepatitis A, B, and C, chlamydia, or mycoplasma +1 - TABLE 4
European Study of Severe Cutaneous Adverse Reactions scoring system for acute generalized exanthematous pustulosisa
Rash Typical Compatible Insufficient Clinical course Yes No Pustules +2 +1 0 Mucosal involvement −2 0 Erythema +2 +1 0 Acute onset < 10 days 0 −2 Distribution/pattern +2 +1 0 Resolution < 15 days 0 −4 Fever > 38.75 °C +1 0 Postpustular desquamation If yes, +1 If no, 0 Polymorphonuclear neutrophils > 7,000/mm3 +1 0 Histology Other disease −10 Not representative, or no histology 0 Exocytosis of polymorphonuclear cells +1 Subcorneal and/or intraepidermal nonspongiform pustule(s) or pustule(s) not otherwise specified (NOS) with papillary edema; or subcorneal and/or intrepidermal spongiform or NOS pustule(s) without papillary edema +2 Spongiform subcorneal and/or intraepidermal pustule(s) with papillary edema +3 ↵a Likelihood of acute generalized exanthematous pustulosis based on total score: ≤ 0 = no; 1–4 = possible; 5–7 = probable; ≥ 8 = definite.
Adapted from information in reference 30.




{kind=link}
{kind=link}
{kind=link}
{kind=link}