


Article Figures & Data
Figures
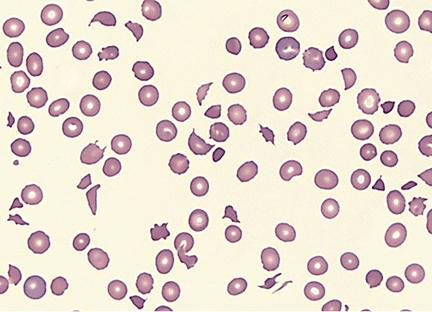
- FIGURE 1
Peripheral blood smear showing microangiopathic hemolytic anemia with numerous schistocytes and thrombocytopenia (Wright-Giemsa, x 500).

Tables
Case 1 Case 2 Reference range Relapse 1 Relapse 2 Age 50 30 38 White blood cell count, × 109/L 16.09 14.16 13.39 3.7–11.0 Hemoglobin, g/dL 5.7 13.6 10.7 11.5–15.5 Platelet count, × 109/L 10 272 32 150–400 Schistocytes Moderate 0 Moderate Lactate dehydrogenase, U/L 2,403 219 718 100–220 Creatinine, mg/dL 0.8 0.8 0.78 0.70–1.40 Fibrinogen, mg/dL 330 253 155 200–400 Activated partial thromboplastin time, seconds 28.7 29.1 26 23.0–32.4 Prothrombin time, seconds 10.9 10 10.9 8.4–13.0 ADAMTS13 activity, % 5 11 <5–9b ≥ 68 ADAMTS13 inhibitor, BUa 0.5 < 0.4 1.8–8b ≤ 0.4 ADAMTS13 antibody, U/mL 18 4 NA <19 Treatment Plasma exchange, prednisone None Plasma exchange, prednisone, dipyridamole, rituximab Follow-up Recent ADAMTS13 activity > 114, platelets 240 Yes 4 months later: ADAMTS13 activity 87, platelets 474 Hemolytic-uremic syndrome Atypical hemolytic-uremic syndrome Disseminated intravascular coagulation and sepsis Idiopathic thrombocytopenic purpura Evans syndrome Malignant hypertension Solid organ or bone marrow transplant Severe vasculitis Pregnancy (preeclampsia, eclampsia, HELLP syndrome) Human immunodeficiency virus infection Liver disease Heavy alcohol intake Disseminated malignancy Drugs (eg, clopidogrel, ticlopidine, cyclosporine, mitomycin C, tacrolimus, quinine, gemcitabine) Combined chemotherapy Total body irradiation Malfunctioning prosthetic cardiac valve Cocaine use HELLP = hemolysis, elevated liver enzymes, and low platelet count
Thrombotic thrombocytopenic purpura Hemolytic-uremic syndrome Ischemia, tissue injury Multiorgan Renal Presentation in children Few cases (early onset of congenital TTP) Most cases; usually accompanied by bloody diarrhea (except in atypical hemolytic-uremic syndrome) ADAMTS13 activity Markedly reduced Normal or mildly reduced in almost all cases Recurrence Common Rare Therapeutic plasma exchange Good response Poor response when associated with Escherichia coli infection May help in atypical hemolytic uremic syndrome Sequelae Approximately 80% of patients showing complete response without sequelae Permanent renal damage in 30% (rate higher in atypical hemolytic uremic syndrome)




{kind=link}