


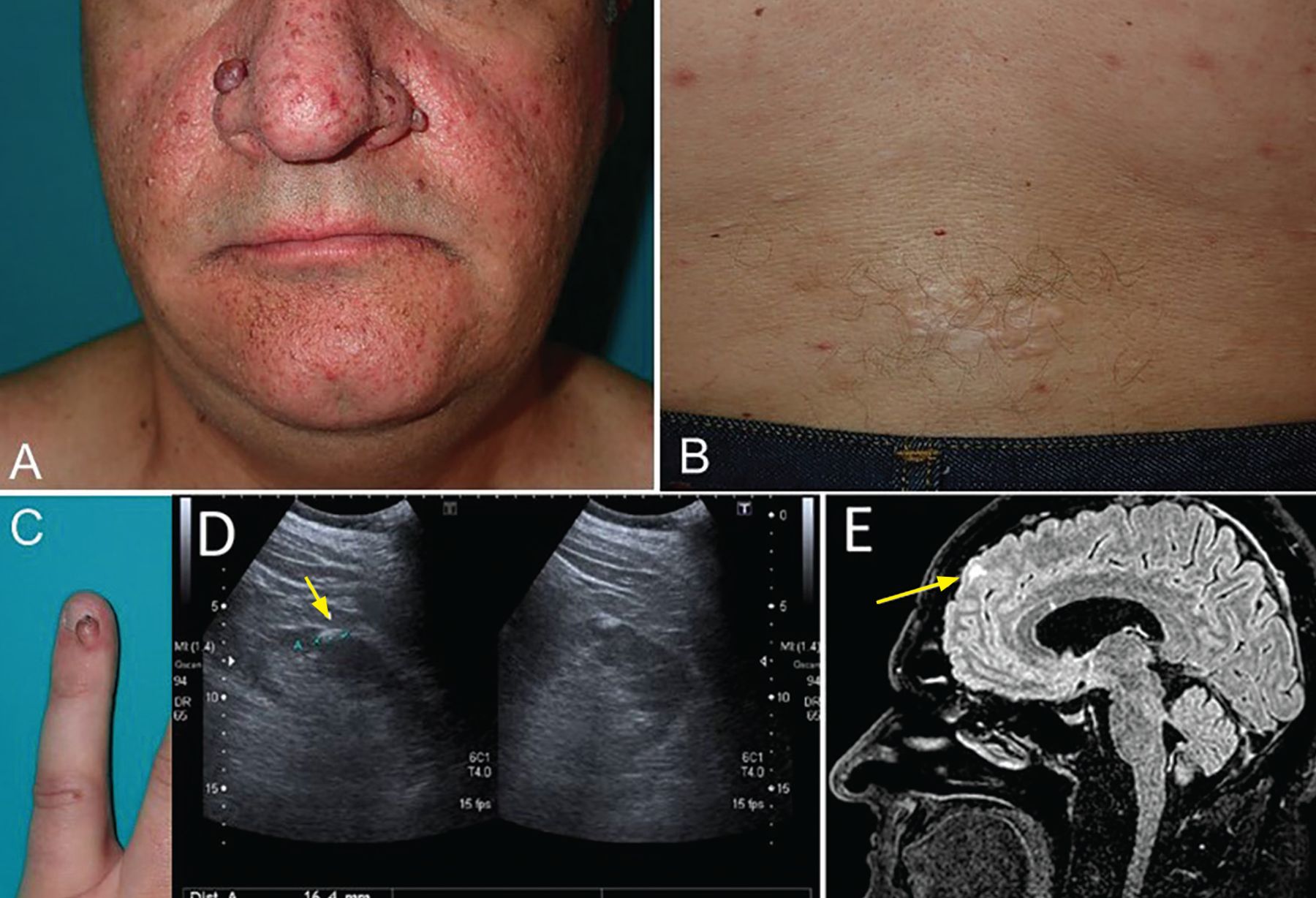
A 45-year-old man with an unremarkable medical history was referred to the dermatology department because of facial lesions. On examination, he had multiple erythematous papules in the malar and nasal regions of the face that were judged to be angiofibromas (Figure 1A). He also had linear hypopigmented macules and shagreen patches on the lower back (Figure 1B) and a periungual fibroma on a fingernail (Figure 1C).

(A) Multiple erythematous papules in the malar and nasal regions were judged to be angiofibromas. (B) Linear hypopigmented macules and shagreen patches were noted over the lower back, as well as (C) a periungual fibroma on a fingernail. (D) Ultrasonography showed a hyperechoic solid lesion compatible with renal angiomyolipoma (arrow). (E) Brain magnetic resonance imaging detected cortical tubers (arrow) as well-circumscribed frontal and occipital areas of high signal intensity on axial fluid-attenuation inversion-recovery.
Although skin lesions such as these can be found in the general population, they can also be associated with certain syndromes. Having 1 or 2 angiofibromas is common in the general population, but multiple facial angiofibromas are present in 80% of patients who have tuberous sclerosis complex (TSC), for which at least 3 lesions are required as a diagnostic criterion. Angiofibromas can also be observed in Birt-Hogg-Dubé syndrome and in multiple endocrine neoplasia type 1.1 Shagreen patches, a type of collagenoma, are present in Cowden syndrome and in approximately half of patients with TSC. Over 90% of patients with TSC have hypopigmented macules, and the differential diagnosis includes postinflammatory hypopigmentation, piebaldism, and vitiligo.1
A genetic test was requested because we suspected TSC detected deletion of the TSC1 gene, and this finding along with findings on the physical examination confirmed the diagnosis of TSC.
Because people with TSC tend to develop tumors in multiple organs of the body, the patient underwent an extensive workup. Ultra sonography of the kidneys showed a hyperechoic solid lesion compatible with renal angiomyolipoma (Figure 1D, arrow), although the patient’s blood test results detected no renal impairment.
Although the patient did not manifest neurologic or neurobehavioral abnormalities, which are common in patients with TSC, brain magnetic resonance imaging detected cortical tubers as well-circumscribed frontal and occipital areas of high signal-intensity on axial fluid-attenuation inversion-recovery images (Figure 1E, arrow), and low signal-intensity on T1-weighted images, interpreted as cortical tubers. An ophthalmic examination, chest radiography, and echocardiography revealed no abnormalities.
SIGNS AND SYMPTOMS
TSC is a rare disorder with an incidence of 1 in 10,000 live births. It is caused by mutations of tumor-suppressor genes, which can lead to benign hamartomas in the brain, eyes, heart, lung, liver, kidney, and skin.2 The most frequent clinical manifestations are dermatologic lesions such as focal hypopigmentation, angiofibroma, ungual fibroma, and shagreen patches,3 but neurologic manifestations such as epilepsy, neuropsychiatric disorders, and behavioral problems are also common. Renal impairment is seen but is not among the most common early clinical manifestations.
Even though benign tumors are more common, there is a risk of malignancy, especially in the brain and kidney.
DIAGNOSIS AND TREATMENT
Appropriate evaluation is important to limit the morbidity and mortality of TSC. Neurologic and renal involvement are the principal causes of morbidity.2 The evaluation should include brain, lung, and abdominal imaging, a complete blood cell count, and pulmonary function testing. The physical examination includes auscultation for heart murmur or lung crackles and identification of eye disorders or abdominal mass.4
Treatment depends on the clinical features. Inhibitors of the mammalian target of rapamycin pathway are a therapeutic option and can be used as adjuvant therapy for large tumors before surgery.5 Other medical treatments depend on the manifestation (eg, antiepileptic drugs in epilepsy). Surgery is considered for solitary lesions that cannot be controlled with conservative treatment in patients without high surgical risk.
OUR PATIENT’S COURSE
The patient was followed by several specialists to monitor for the appearance of complications, occasionally requiring resection of a skin lesion with local complication.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.