


ABSTRACT
Although orthostatic hypotension is common and can have serious consequences, recommendations about its evaluation and management are based on limited data. Here, the author outlines a systematic approach, noting the areas that pose an opportunity for improvement.
The diagnosis of orthostatic hypotension must be systematic. Do not assume causality. For example, if the patient has diabetes mellitus and orthostatic hypotension, do not assume that diabetic autonomic neuropathy is the cause of the orthostatic hypotension.
When evaluating the cause of orthostatic hypotension, consider the tempo of progression of disease and the coexistence of neurologic symptoms.
Treatment should first focus on nondrug therapy, but when adding drug therapy such as fludrocortisone and vasoconstrictors, consider volume status and the presence or absence of supine hypertension.
Supine hypertension is common in neurogenic orthostatic hypotension. It should be treated by discontinuing fludrocortisone and long-acting antihypertensives. Elevation of the head of the bed, high-carbohydrate snacks at bedtime, and short-acting antihypertensive drugs at bedtime, preferably nitrates or clonidine, can be useful.
An 83-year-old woman was transferred from another hospital because of refractory orthostatic hypotension (OH) and recurrent syncope for the past 3 months. She had been healthy through her life other than for well-controlled hypertension and hyperlipidemia. She lived independently and was very functional. On admission, she could not stand for more than 1 to 2 minutes because of severe presyncopal dizziness. Her review of systems was otherwise negative, aside from frontal headaches that happened primarily when her blood pressure (BP) was high, and constipation, which had been worse recently.
Her medications at the time of transfer included midodrine 10 mg three times a day, fludrocortisone 0.1 mg daily, and atorvastatin.
Supine, her BP was 172/94 mm Hg and her heart rate (HR) was 64 beats per minute. Sitting, her BP dropped to 108/72 mm Hg with an HR of 76 beats per minute. After standing for 1 minute her BP dropped to 66/42 mm Hg while her HR increased only to 84 beats per minute. She immediately sat down because of presyncopal dizziness. Other findings on examination, including a complete neurologic examination by a neurologist, were unremarkable.
She had already undergone many tests with normal results. These included a complete metabolic panel; complete blood cell count; thyroid function tests; urinalysis; electrocardiography; echocardiography; chest radiography; brain magnetic resonance imaging; auto-antibody serologic testing (antinuclear antibody, Sjögren syndrome antibody A, Sjögren syndrome antibody B); tests for human immunodeficiency virus, Lyme disease, hepatitis B, and hepatitis C; vitamin B profile; vitamin D levels; and serum protein electrophoresis and free circulating light chains.
Which is the most appropriate next diagnostic test for this patient?
Formal autonomic nervous system testing
Serum paraneoplastic and autoimmune neuroautoantibody panel
Abdominal fat pad biopsy
Electromyography and nerve conduction studies
Skin biopsy to measure nerve fiber density.
The answer lies in an understanding of OH and key elements of the evaluation.
ORTHOSTATIC HYPOTENSION DEFINED
OH is present if the systolic BP drops by more than 20 mm Hg or the diastolic BP drops by more than 10 mm Hg.1 The systolic BP is preferred because it has better association with cerebral blood flow and symptoms.2,3 If the patient is hypertensive, then a systolic drop of more than 30 mm Hg is the threshold.1
ADAPTATION TO STANDING
When we stand up, gravitational forces lead to blood pooling in veins of the lower body, amounting to about 500 to 800 mL. About 50% of the pooling occurs in the thighs, 25% in the lower legs, and 25% in the pelvis. Given the increased venous hydrostatic pressure, plasma fluid leaks into the interstitial space, leading to a modest (10%–15%) decrease in plasma volume, decreased BP, and decreased pulse pressure (a useful marker of decreased stroke volume). These hemodynamic changes lead to decreased arterial baroreceptor firing, which in turn leads to increased sympathetic tone and decreased parasympathetic tone. This immediate response is what leads to the appropriate responses of tachycardia, arterial vasoconstriction, venoconstriction, and increased cardiac contractility. There are also increases in antidiuretic hormone and angiotensin II, but these take longer to take effect. In short, the immediate adaptations to orthostatic stress are primarily mediated by enhanced sympathetic activity.
OH develops when these compensatory measures fail. OH is very common, affecting up to 30% of ambulatory patients, especially at older age. Hospitalized patients also have high rates, particularly transient OH related to immobility and volume depletion. OH causes troublesome symptoms such as orthostatic dizziness and lightheadedness, fatigue, visual blurring, muffled hearing, pain in the neck and shoulders (“coat-hanger” symptoms), and impaired concentration, as well as syncope and falls, often with injuries. However, many patients are completely asymptomatic despite severe reductions in BP.3 A meta-analysis of available observational cohorts showed that OH is associated with significantly increased risk of death (risk ratio 1.50), coronary disease (risk ratio 1.41), stroke (risk ratio 1.64), and heart failure (risk ratio 2.25).4 Despite extensive observational data identifying these risks, there are no clinical trials demonstrating that this risk can be modified by therapy.
EVALUATION OF ORTHOSTATIC HYPOTENSION
Following appropriate procedure is essential for accurate identification of OH. BP and HR are measured with the patient supine after at least 5 minutes of supine rest.1 The patient then is tilted up or, in the office, the patient stands up, and BP and HR are measured at 1 minute and 3 minutes. Seated measurements are not needed, although I often obtain them to allow patients with severe OH to adapt before standing, and knowledge of seated BP levels is important as part of monitoring patients under treatment.
Supine BP values are useful to identify supine hypertension (see discussion below). Standing values provide us a measure of the severity of OH. In treated patients, measurements at the peak of action of drugs assess the effectiveness of therapy. Seated values, on the other hand, serve as a marker of safety as they identify both hypotension in untreated patients and excessive BP elevation in patients with treated OH.
Is there an appropriate heart rate response?
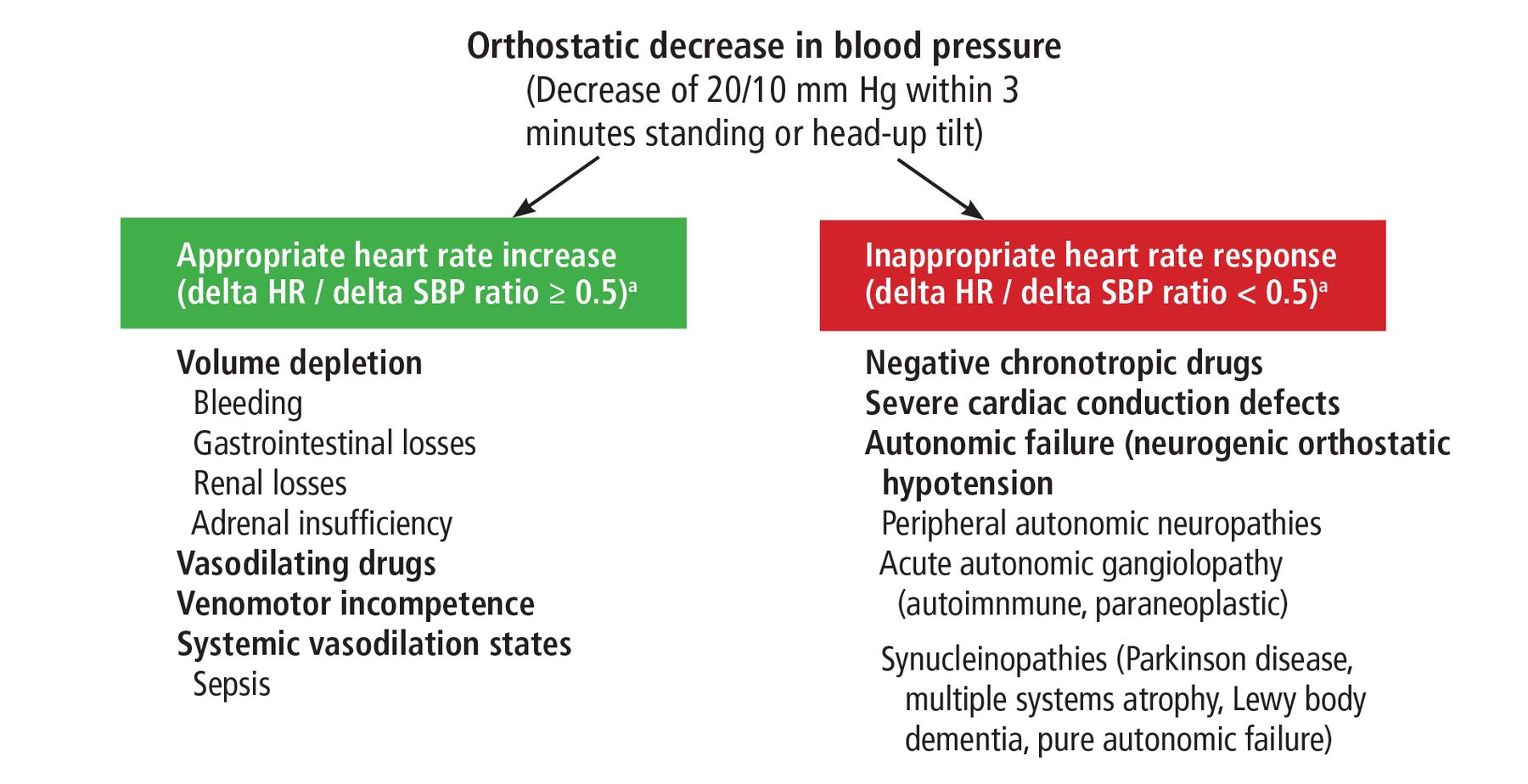
If the patient has OH, the first and critical question is whether there is an appropriate HR response (Figure 1).
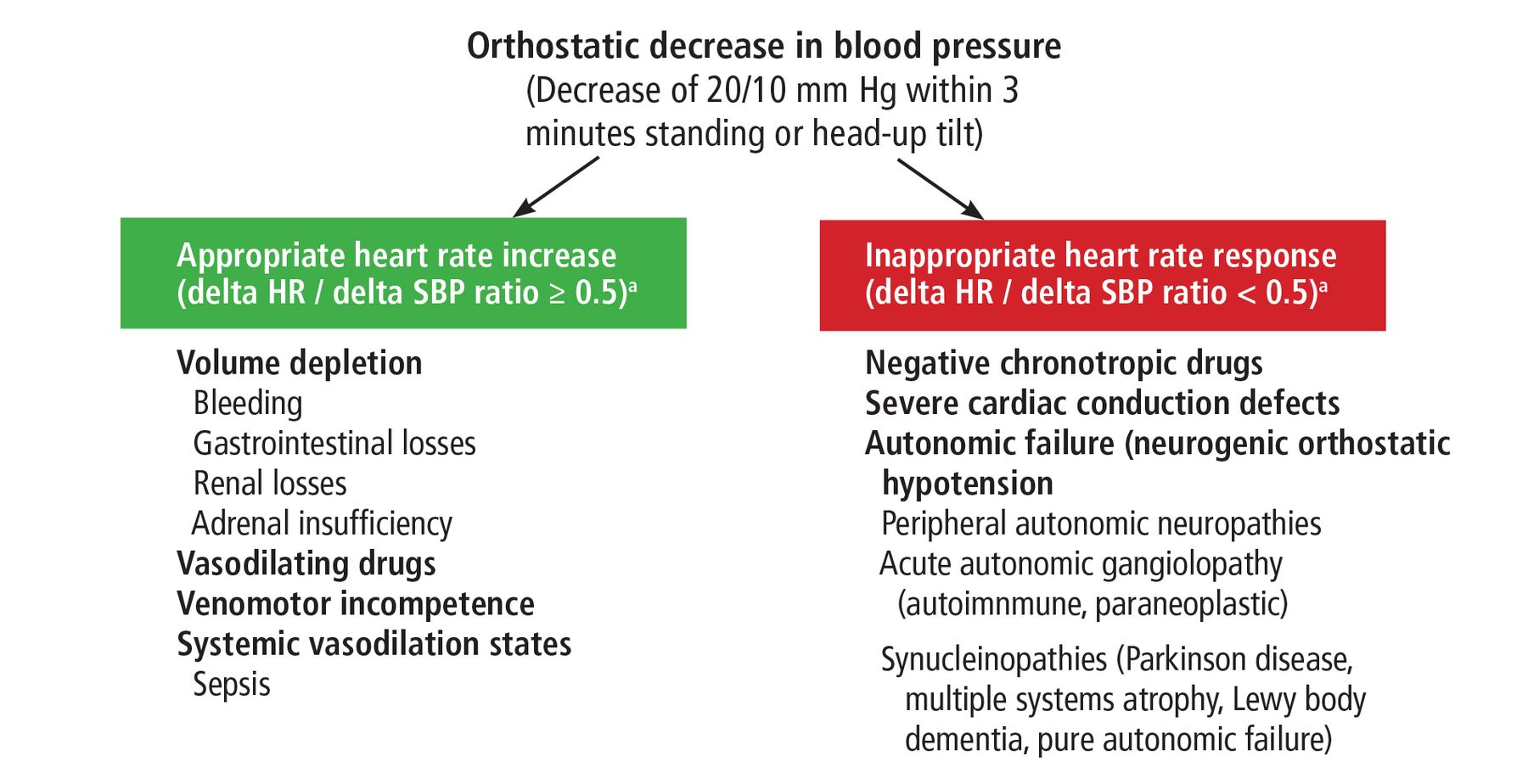
Diagnostic approach to orthostatic hypotension.
a Delta HR/delta SBP ratio is the ratio of the change in heart rate divided by the change in systolic blood pressure with standing or head-up tilt. Most patients with neurogenic orthostatic hypotension have a ratio below 0.3. Most patients with a normal autonomic response have a ratio above 1.0.
As BP falls, the HR should increase in response. An appropriate HR response is defined by the ratio of the change in HR to the change in systolic BP with head-up tilt or standing.5,6 In patients with intact autonomic responses, this ratio is greater than 0.5: for example, if the systolic BP falls by 40 mm Hg, a normal HR response should be an increase of greater than 20 beats per minute.6 A ratio less than 0.5 identifies a neurogenic component with good sensitivity (91%) and specificity (88%).6
Use of this ratio is an important recent advance in the evaluation of OH, though a recent study corroborated its sensitivity but demonstrated very low specificity (50%).7 Therefore, it is likely that further refinement of the procedure will be needed.
If there is an appropriate HR response, think of common causes, such as volume depletion of any cause, vasodilator drugs, venomotor incompetence (very often associated with immobility), or systemic vasodilatory states.
If the HR response is inadequate, possibilities include the use of a negative chronotropic drug (eg, beta-blocker, verapamil, diltiazem, ivabradine), the presence of a cardiac conduction defect (easily identified by an electrocardiogram and often requiring a pacemaker for effective management), or autonomic failure (neurogenic OH).
What are the neurogenic causes of orthostatic hypotension?
Autonomic neuropathy is a common cause of neurogenic OH. Possible etiologies of autonomic neuropathy are too numerous to list but include diabetes mellitus, amyloidosis, toxic neuropathies (drugs, heavy metals), infections, autoimmune diseases, hereditary conditions, paraneoplastic syndromes, and metabolic disorders. Table 1 provides a summary of the most common causes of peripheral autonomic neuropathies to help guide further diagnostic testing based on clinical plausibility.
Relevant causes of peripheral autonomic neuropathies to help guide the diagnostic evaluation
An approach to sorting out the neurogenic causes of OH involves considering the type of associated neurologic findings (if any) and whether the onset of the OH was acute/sub-acute or chronic and progressive.8 Using this approach, the following 5 distinct categories arise:
No neurologic symptoms, acute or sub-acute onset (less than 3 to 6 months). Consider autoimmune or paraneoplastic ganglionopathy and toxic exposures, particularly neurotoxic drugs. These cases often go undiagnosed. It is essential that these conditions be identified because they often have specific therapy, such as immunomodulatory therapy for autonomic ganglionopathies or removal of a potentially toxic drug.
No neurologic symptoms, chronic, slow progression. Consider pure autonomic failure, a synucleinopathy that usually presents without nonautonomic features but often progresses to Parkinson disease or multiple system atrophy after prolonged follow-up.9
Extrapyramidal or cerebellar motor features, chronic progressive course. Consider synucleinopathies such as Parkinson disease, Lewy body dementia, and multiple system atrophy (with parkinsonian or cerebellar features).
Peripheral neuropathic symptoms, acute or subacute onset. Consider paraneoplastic syndromes, Sjögren syndrome and other connective tissue diseases, and toxic exposures.
Peripheral neuropathy, chronic progressive onset. Consider diabetes, amyloidosis, autoimmune disorders, infections, toxic exposures, and metabolic or hereditary disorders.
Diagnostic testing
A review of systems should look for causes of volume depletion, infection, and heart disease in addition to specific nonautonomic neurological symptoms (particularly extrapyramidal, cerebellar, or peripheral sensorimotor).
Vital signs should be taken in the office and at home. As part of the initial evaluation, I ask patients to keep a log of orthostatic BP at home for 1 to 2 weeks. I instruct them to measure BP at the following times:
Upon getting up in the morning before taking any medications; this informs us of the presence and magnitude of supine hypertension and helps quantify the severity of the orthostatic hypotension
After meals, because postprandial hypotension is common, and meal content may need to be modified (less rich in carbohydrates)
If applicable, after vasopressor doses (1 to 2 hours after midodrine or droxidopa) to assess the effectiveness and safety of the treatment
In the evening, to assess BP changes throughout the day. Most patients with neurogenic OH tend to have higher BP and less OH in the afternoon and evening.
Additionally, 24-hour BP monitoring can be useful to assess for nighttime supine hypertension and overall BP control. This is particularly useful in patients with significant BP changes from supine to seated to standing positions.
A detailed medication review should identify drugs that may lower BP or predispose to OH. These include antihypertensives, diuretics, anticonvulsants, antipsychotics, antidepressants, opioids, and benzodiazepines.
Testing includes electrocardiography, complete blood cell count, complete metabolic panel, thyroid function tests, and urinalysis for all patients. Patients without obvious neurologic findings often undergo further testing guided by the nature of the findings. Many patients benefit from echocardiography to rule out pericardial disease, pulmonary hypertension, severe valvular disease (especially aortic stenosis), and left ventricular dysfunction. Likewise, a cosyntropin stimulation test may be done to rule out adrenal insufficiency.
Many other tests have limited data to support them but may be used creatively in the management of complex cases. For example, I often use bioimpedance to objectively measure extracellular fluid volume when unsure of the level of volume repletion in a patient, allowing me to adjust some of the treatments that target volume expansion (salt tablets, fludrocortisone). Likewise, autonomic testing equipment with beat-to-beat BP monitoring can provide hemodynamic data (stroke volume, cardiac output, peripheral resistance) that can help guide adjustments in medications. The equipment I use for autonomic testing (Finapres NOVA) has a hemodynamics module useful in complex cases, though this approach has only been used anecdotally and has not been tested in clinical trials.
A detailed autonomic evaluation using beat-to-beat BP and HR monitoring (during tilt and Valsalva maneuver) and quantitative sweat responses may have value. But usually, when patients present with OH due to autonomic failure, the diagnosis is obvious, and autonomic testing usually adds little.
Electromyography, nerve conduction studies, skin biopsy to quantify nerve fiber density and identify amyloid fibrils (and possibly alpha-synuclein), and targeted serologic evaluation can be of value in the evaluation of patients with peripheral neuropathic findings.
Brain imaging is always done for patients with motor findings and includes magnetic resonance imaging. Sometimes magnetic resonance or computed tomographic angiography of the head and neck may be useful to evaluate the vertebrobasilar circulation in patients who develop severe orthostatic symptoms at BP levels that are not very low (eg, systolic BP > 120 mm Hg).
A dopamine transporter scan may be of value to confirm a diagnosis of Parkinson disease, multiple system atrophy, or dementia with Lewy bodies.
Finally, cardiac 123I-meta-iodobenzylgua-nidine scintigraphy or 18F-fluorodopamine positron emission tomography may help distinguish between multiple system atrophy and Lewy body synucleinopathies (Parkinson disease and Lewy body dementia). In the former, there is preserved cardiac autonomic innervation, whereas in Parkinson and Lewy body dementia, cardiac uptake of catecholamines is decreased.10
MANAGEMENT OF ORTHOSTATIC HYPOTENSION
Patients with nonneurogenic causes of OH can usually be managed with treatment of underlying disorders, removal of offending agents, and volume replacement. Likewise, a pacemarker may be needed for patients with qualifying conduction defects.
Most causes of OH requiring long-term treatment are neurogenic. A consensus panel assembled by the American Autonomic Society and the National Parkinson Foundation recommends a stepwise approach to the treatment of neurogenic OH.11
Step 1 is a detailed medication review to identify drugs that often cause OH. Long-acting antihypertensives almost always should be stopped. When absolutely needed, administration should be at night. Antidepressants and anticonvulsants may have to be reconsidered.
Step 2 is the addition of nonpharmacologic measures. Exercise increases muscle tone and improves venomotor competence, reducing venous pooling, but should be either recumbent (eg, on a recumbent bike or rowing machine) or aquatic (swimming or pool-walking) to maximize tolerability.
I recommend high sodium (> 150 mEq/day) and fluid (at least 2 L/day) intake to most patients. A premeal water load such as drinking 500 mL of water in about 5 minutes can be useful, especially if the patient has significant postprandial symptoms. In patients with autonomic failure, there is a significant increase in BP for 60 to 90 minutes in response to the osmosympathetic reflex whereby a decrease in osmolality of splanchnic blood results in an increase in sympathetic tone.12
I also recommend external venous compression to all patients. Compression stockings should ideally come up to the waist to maximize the extent of compressed venous territory. Because the venous pressure at the level of the hips is about 30 mm Hg, patients should preferably wear garments that have a “30-40 gradient” (30 mm Hg at the thigh or waist and 40 mm Hg at the ankle), but some patients cannot tolerate the compression due to discomfort. In addition, some patients cannot get them on, so a compromise with lower compression garments (20-30 mm Hg or 15-20 mm Hg) is often needed. Most patients tolerate waist-high garments except for those who have urinary frequency or significant abdominal bloating or pain.
Step 3 is drug treatment. Despite the absence of high-quality evidence to support their use,13,14 the cornerstone drugs are fludrocortisone, midodrine, and droxidopa; pyridostigmine and atomoxetine are used less often. Table 2 summarizes relevant pharmacologic and clinical features of these agents. Only midodrine and droxidopa are approved by the US Food and Drug Administration (FDA) for use in OH. All other medications are used off-label.
Key drugs used in treating orthostatic hypotension
Fludrocortisone is a synthetic mineralocorticoid that increases extracellular fluid volume and increases sensitivity to catecholamines.15 Because of its long duration of action, sustained hypertension (particularly at night) is often a problem limiting its use.
The vasoconstrictors midodrine and droxidopa are short-acting and therefore more useful for treatment during the daytime while avoiding supine hypertension at night. In one study, midodrine significantly increased the time to development of syncope or near-syncope on tilt testing by about 600 seconds, though not all patients responded.16 Droxidopa is less potent than midodrine, but it does cause a significant increase in BP compared with placebo, along with a decrease in orthostatic symptoms.17,18
Midrodine and droxidopa have never been compared against each other, but individual patients respond differently. Some have a greater response to midodrine than to droxidopa, and some, the reverse. We do not yet know the reason for these differences nor can we predict how patients will respond, so in practice, if one drug does not work well, I try the other. Combining droxidopa and midodrine has not been formally tested. Anecdotal experience has been at times successful.19
Pyridostigmine is an acetylcholinesterase inhibitor that increases cholinergic transmission in autonomic ganglia and peripheral nerves. It has a modest and inconsistent effect on OH.20,21 The ganglionic effect increases sympathetic tone, particularly in response to orthostatic stress, thus limiting the occurrence of supine hypertension.
Atomoxetine is a selective norepinephrine transporter inhibitor with inconsistent effects on orthostatic BP,22 but in one recent study it was noted to improve standing BP similarly to midodrine while producing marginally larger improvements in orthostatic symptoms.23
Other medications used much less frequently, usually as last options when nothing else works, include octreotide, erythropoietin, desmopressin, pseudoephedrine, and ergot derivatives.13
My opinion-based approach to initial therapy. If the patient has no supine hypertension, I start with either a vasoconstrictor or fludrocortisone. I prefer vasoconstrictors not only because they are FDA-approved, but also because they can be used on an as-needed basis to treat intermittent symptoms, which is often the case, especially in patients with mild disease or early in the course of a progressive disease. If patients have no heart failure, edema, or hypokalemia, one can use either fludrocortisone or a vasoconstrictor, but the presence of any of these conditions argues against using fludrocortisone. I use pyridostigmine as the first choice only if a patient has mild neurogenic OH and significant constipation or gastroparesis, as it allows me to treat both the OH and the gastrointestinal hypomotility.
Step 4. Fludrocortisone and a vasoconstrictor can be combined. If the patient is already receiving both, then pyridostigmine or atomoxetine can be added.
Importantly, most of the trials to support the above treatments are small, uncontrolled observational studies. There is much need for improvement. For example, we have no drugs to specifically target the impaired venomotor tone. Perhaps a drug that blocks the natriuretic peptide receptor could cause valuable venoconstriction—picture it as the opposite of a nitrate or nesiritide. Alternatively, non-catecholamine vasoconstrictors (vasopressin, angiotensin II) are available for intravenous use in critically ill patients, but these are not yet translated to viable oral options that could be used to treat neurogenic OH. Desmopressin is a vasopressin V2-receptor agonist with limited pressor function. Its modest favorable effects in neurogenic OH are likely related to decreased nocturnal urine output, not vasoconstriction. Terlipressin, on the other hand, is a potent vasopressin V1-receptor agonist used in patients with hepatorenal syndrome. It has a potent pressor effect in patients with neurogenic OH when given intravenously24 but is not available in oral form. Additionally, and very importantly, we do not know the long-term impact of therapy on patient-reported outcomes, functional outcomes (injurious falls, syncope, cognition), or cardiovascular outcomes.
SUPINE HYPERTENSION
Supine hypertension is a common complication of OH, affecting 40% to 70% of patients, adding complexity to patient management. It is graded as mild if the supine BP is 140–159/90–99 mm Hg, moderate if 160–179/100– 109 mm Hg, and severe if 180/100 mm Hg or higher, as measured after at least 5 minutes of supine rest.25 I usually accept supine BPs up to 160/100 mm Hg, and depending on the severity of the OH, I may be forced to accept pressures as high as 180 mm Hg. In such cases, 24-hour BP monitoring is extremely helpful to quantify the overall BP burden.
The approach to its treatment is first non-pharmacologic. Fludrocortisone should almost always be stopped. Vasopressors should not be given within 4 to 6 hours before going to bed. Elevation of the head of the bed, typically about 8 inches, is helpful but often not well tolerated. If using an adjustable mattress, the head of the bed is elevated about 30 degrees and, if adjustable, the foot of the bed is lowered by a similar amount. Also, if the presence of diabetes or obesity does not prohibit it, I often recommend a high-carbohydrate snack at bedtime if patients have a demonstrable response to it. The typical effective dose is 200 to 400 calories (50–100 g) in the form of pure carbohydrates, eg, candy. Sensitivity varies, and many patients have a good response to smaller doses.
Pharmacologic management is often needed.26 Because of the problem of OH during the day, long-acting agents cannot be used. Short-acting antihypertensive drugs are given at bedtime. Several agents can effectively lower BP, but my personal preference for initial use is nitrates. Most of the studies have used topical nitroglycerin,27 though to avoid hypotension, patients have to wake up early to remove the patch and stay in bed for 30 to 60 minutes before getting up. Because of this, I prefer isosorbide dinitrate (starting dose 20 mg, titrated up to 80 mg as needed).
Clonidine (0.1 mg orally) and nitroglycerin lower nighttime BP to a similar degree, but nitroglycerin has less residual BP-lowering effect in the morning.27 Clonidine is often helpful in patients with residual sympathetic tone, which is most commonly observed in patients with multiple system atrophy.
Other drugs tested in single-dose trials include sildenafil, captopril, losartan, nebivolol, eplerenone, minoxidil, and hydralazine, with variable results and often a “tail effect” in the morning.26 Even though losartan is relatively long-acting, surprisingly it does not worsen morning OH, presumably due to increased angiotensin II levels.28 It is a drug I prescribe often, particularly in patients with chronic kidney disease or heart failure with reduced ejection fraction, in whom the use of a blocker of the renin-angiotensin system has significant benefits.
CASE CONCLUDED
In our patient, the rapid pace of development raised the concern for an acute autonomic ganglionopathy. Acute autonomic neuropathy is called ganglionopathy because the lesion is at the autonomic ganglia.29 This is a rare disorder in which patients present with acute or subacute pandysautonomia (orthostatic hypotension, neurogenic bladder, gastrointestinal hypomotility, pupillary dysfunction, hypohidrosis) in various combinations. It is typically immunemediated and can be transferred passively in animal models. The initial description was caused by antibodies against the ganglionic acetylcholine alpha 3 receptor.30 These antibodies have also been described in paraneoplastic autonomic ganglionopathy, although in that condition the most common antibody is the antineuronal nuclear antibody type 1 (ANNA-1, formerly called anti-Hu antibody).29 These antibodies are tested using commercially available neuroautoantibody panels. Several other rare antibodies have been described, and 30% to 50% of patients presenting with the classic syndrome are seronegative. The severity of the elevation of antibody titers often correlates with the clinical presentation. It is likely that seronegative patients have antibodies against epitopes not yet identified, as many improve with immunomodulatory treatments.31 Treatments reported include plasma exchange, intravenous immunoglobulin, and a variety of immunosuppressants.29,32 Our protocol includes intravenous immunoglobulin with or without steroids.
Given this possibility in our patient, we obtained a neuroautoantibody panel (Mayo Clinic Laboratories). The patient had moderately high titers of antibody against the ganglionic acetylcholine receptor. Given her age, we suspected a paraneoplastic syndrome despite a lack of symptoms, but no tumor was identified on computed tomography (neck to pelvis), in addition to a normal recent colonoscopy. Sometimes the syndrome presents before a malignancy is clinically identifiable. However, in its absence, we diagnosed her as having autoimmune autonomic ganglionopathy with predominant cardiovascular involvement (and perhaps mild gastrointestinal disease, given the constipation). We treated her with intravenous immunoglobulin (2 g/kg over 5 days) and intravenous methylprednisolone (500 mg/day for 5 days). She had a positive response and was able to walk out of the hospital and to attend rehabilitation 3 weeks after treatment was started. She remained on biweekly intravenous immunoglobulin for 2 months and on monthly doses for another 4 months. She continued to have OH but regained reasonable orthostatic tolerance and returned to independent living on maintenance therapy with midodrine 5 mg 2 to 3 times daily. Her current orthostatic tolerance is in the range of 7 to 10 minutes.
As for the other possible answers to the question regarding the most appropriate test for our 83-year-old patient, autonomic testing would not have given additional information. Amyloid was not likely based on the rapid rate of progression (ie, within 3 months) and the negative screen for AL amyloid. Hereditary amyloid forms and AA amyloid were clinically improbable. Electromyography and nerve conduction studies would probably not have helped as the patient had no peripheral sensorimotor findings. Skin biopsy could be useful to identify decreased nerve fiber density as seen in small fiber neuropathies, but the presentation did not suggest this.
DISCLOSURES
Dr. Peixoto has disclosed research/independent contracting for Bayer, Boehringer-Ingelheim, Lundbeck, and Vascular Dynamics; serving as advisor or review panel participant for Ablative Solutions and Relypsa Pharmaceuticals; and serving as consultant/advisor or review panel participant for Diamedica Therapeutics. This presentation discusses off-label-use of medications: fludrocortisone, pyridostigmine, octreotide, and atomoxetine.
Footnotes
Medical Grand Rounds articles are based on edited transcripts from Medicine Grand Rounds presentations at Cleveland Clinic. They are approved by the author but are not peer-reviewed.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.