


Article Figures & Data
Figures
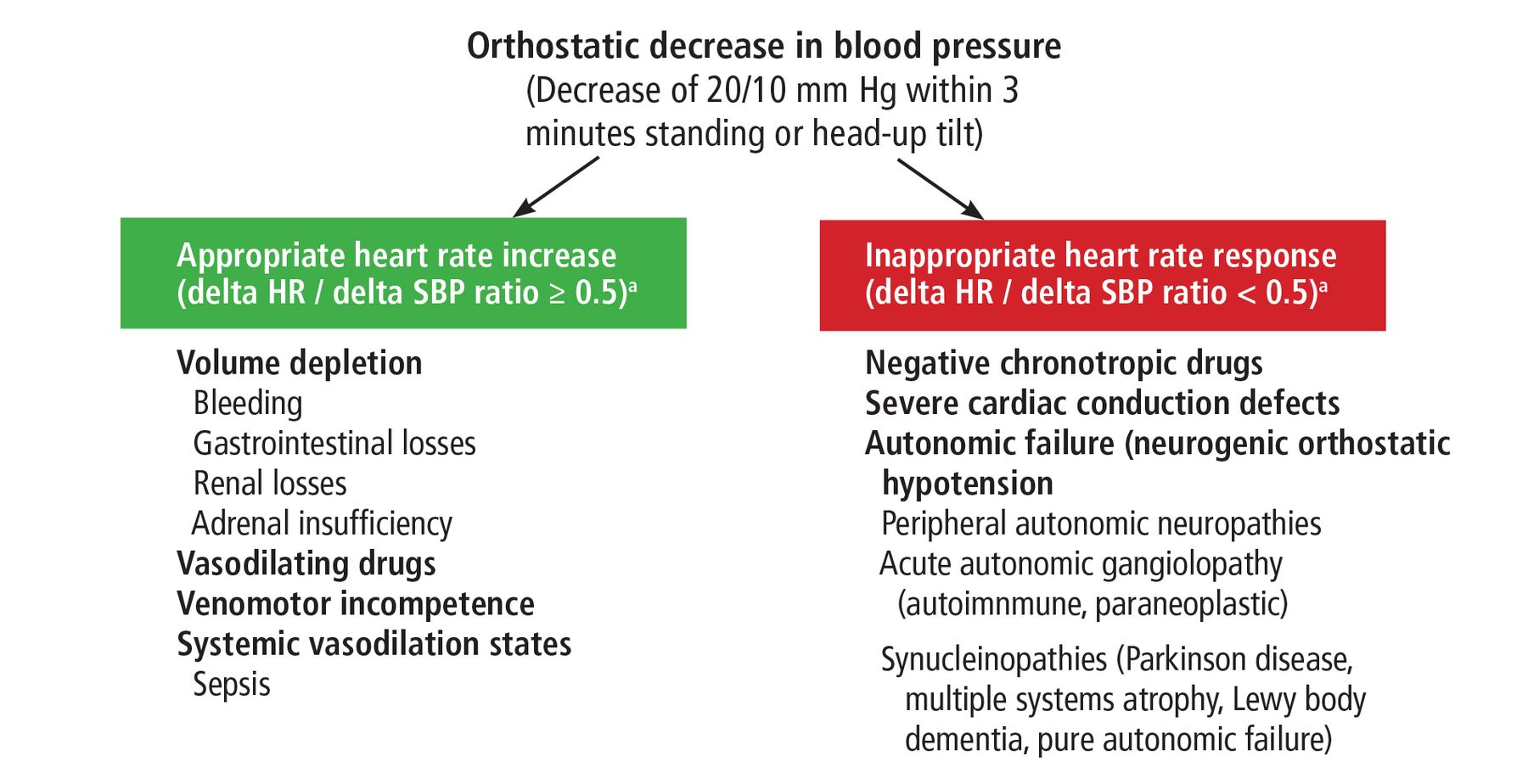
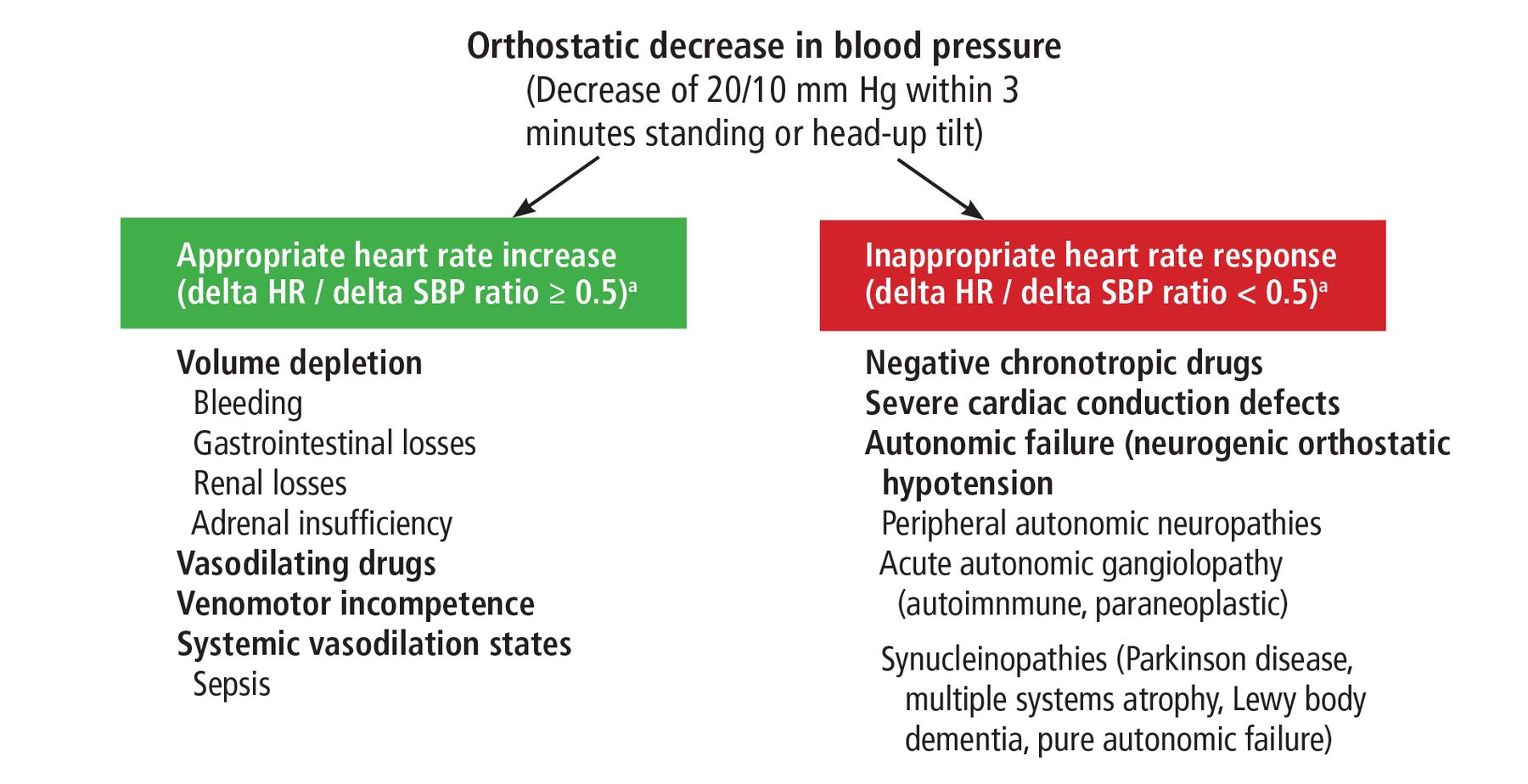
- Figure 1
Diagnostic approach to orthostatic hypotension.
a Delta HR/delta SBP ratio is the ratio of the change in heart rate divided by the change in systolic blood pressure with standing or head-up tilt. Most patients with neurogenic orthostatic hypotension have a ratio below 0.3. Most patients with a normal autonomic response have a ratio above 1.0.
Tables
- TABLE 1
Relevant causes of peripheral autonomic neuropathies to help guide the diagnostic evaluation
Diabetes mellitus Amyloidosis
AA (secondary) amyloidosis
AL (light chain, primary) amyloidosis
Transthyretin and other hereditary formsToxins
Heavy metals
Vincristine
Paclitaxel
Cisplatin
Thalidomide
BortezomibInfections
Human immunodeficiency virus
Chagas disease
Leprosy
Botulism
Diphtheria
Lyme disease
SyphilisAutoimmune
Sjögren syndrome
Systemic lupus erythematosus
Mixed connective tissue disease
Sarcoidosis
Acute inflammatory demyelinating polyneuropathy
Chronic inflammatory demyelinating polyneuropathyHereditary
Hereditary peripheral and autonomic neuropathy
Fabry disease
Allgrove syndromeParaneoplastic Metabolic
Renal failure
Hypothyroidism
Vitamin B12 deficiency
Porphyria Drug Class Advantages Disadvantages Comments Fludrocortisone Synthetic mineralocorticoid Increases extracellular volume and blood pressure
Increases sensitivity to catecholaminesSupine hypertension
Edema
Long-acting (half-life 18–36 hours)Start at 0.1 mg daily; increase to 0.2 mg after 2 weeks
Onset of action is not immediate; full effect takes several days to 1 weekMidodrine Prodrug of desglymidodrine (a direct alpha-1 agonist) Increases arterial and venous tone and blood pressure Short-acting (half-life 3–4 hours) Supine hypertension
Urinary retentionStart with 2.5 mg three times a day (TID) (early morning, lunchtime, late afternoon); avoid doses within 4–6 hours before bedtime
Increase dose by 2.5 mg TID every 3–7 days until symptoms controlled or maximum dose of 10 mg TID reached
Higher doses are approved for other indications, but there is a flat dose-response curve at doses above 10 mgDroxidopa Precursor of norepinephrine (after conversion by dopa decarboxylase) Increases arterial and venous tone
Short-acting (half-life 2.5 hours)Supine hypertension Start with 100 mg TID (early morning, lunch-time, late afternoon)
Avoid doses within 4–6 hours before bedtime
Increase dose by 100 mg TID every 3–7 days until symptoms controlled or maximum dose of 600 mg TID reachedPyridostigmine Anticholinesterase Improves standing blood pressure without change in supine blood pressure Short-acting (half-life 3–4 hours) Wheezing
Abdominal pain
Diarrhea
HyperhidrosisUseful in patients with constipation with or without urinary hesitancy
Start with a 30-mg test dose; if well tolerated, give 60 mg twice a day, increasing to TID after 1–2 weeks if tolerated
Seldom used at doses > 90–120 mg TID
Titrations made every 1–2 weeksAtomoxetine Selective norepinephrine reuptake inhibitor Increases standing blood pressure Supine hypertension
Irritability
Insomnia
Aggressive behavior
Suicidal ideationUsed in lower doses than for attention deficit hyperactivity disorder
Start at 10 mg once daily in morning, increasing to 18 mg, then 25 mg once daily
Higher doses avoided, though safe to use up to 50 mg daily
Titrations made every 1–2 weeks
Half-life 5 hours, active metabolites 6–8 hours
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.