


ABSTRACT
Cardiovascular events have a major impact on overall outcomes after liver transplantation. Today’s transplant patients are older than those in the past and therefore are more likely to have coexisting cardiac comorbidities. In addition, pathophysiologic effects of advanced liver disease on the circulatory system pose challenges in perioperative management. This review discusses important preoperative, intraoperative, and postoperative cardiac considerations in patients undergoing liver transplant.
The average age of patients undergoing liver transplant has risen over the years, and a greater percentage than in the past now have nonalcoholic steatohepatitis as their underlying diagnosis.
Cardiac evaluation and optimization before liver transplant is crucial to avoid adverse clinical outcomes. This should ideally be done by a dedicated cardiology team with experience and expertise in managing cardiac issues pertinent to this specific population.
Outcomes after liver transplant have improved over time even though the patients are at higher risk.
The clinical outcomes of liver transplant recipients might be further improved preoperatively with standardized cardiac risk-stratification pathways, and perioperatively with evidence-based cardiac clinical care. This is an evolving field, and more research is needed to guide clinical decision-making in several important areas of clinical care.
Attention to the heart before, during, and after liver transplantation can pay off in terms of better outcomes. This, even though today’s liver transplant patients are older than those in the past and more likely to have fatty liver disease as the cause of their liver failure, and even though liver failure, the transplant procedure, and the post-transplant regimen can all predispose to heart disease.
The changing demographics of patients receiving liver transplants and the unique cardiac pathophysiology of patients with advanced liver disease pose significant challenges in managing these patients perioperatively, as we will discuss in the following sections.
OLDER PATIENTS, MORE FATTY LIVER DISEASE
Liver transplant is currently the second most common organ transplant in the United States, after kidney transplant. The number of liver transplants per year has increased greatly over time, from 1,713 in 1988 to 8,906 in 2020.1
At the same time the age of patients receiving transplants has also increased. For instance, 476 (28%) of the 1,713 liver transplant recipients in 1988 were age 50 or older, increasing to 6,497 (73%) of 8,906 in 2020.1 Survival rates are lower in older patients: 75.0% at 5 years in those age 35 to 49, 70.9% in those age 50 to 64, but only 65.9% in those 65 and older,1 likely due to more comorbidities such as coronary artery disease in the older patients.
Another important change in patients receiving liver transplants has been an increase in those with nonalcoholic steatohepatitis as the underlying diagnosis. In 2013, nonalcoholic steatohepatitis was the second most common cause of liver failure in new wait-list registrants for liver transplant, after hepatitis C cirrhosis.2
Patients with nonalcoholic steatohepatitis typically have traditional risk factors for coronary artery disease such as diabetes mellitus, obesity, hypertension, and hyperlipidemia,3 and thus have a higher risk of coronary artery disease.4 After liver transplant, cardiovascular events are much more common in patients with nonalcoholic steatohepatitis than in those with other causes of liver failure.5
HEART DISEASE IN LIVER TRANSPLANT RECIPIENTS
Liver transplant recipients have a higher prevalence of coronary artery disease than in the general population. Other important cardiac conditions to recognize and manage include cirrhotic cardiomyopathy, portopulmonary hypertension, heart failure, and thromboembolism.
Coronary artery disease
In various studies,6–8 the prevalence of coronary artery disease in patients with end-stage liver disease has ranged from 16.2% to 27%, which is higher than in the general population (6%)9 and similar to that in patients with diabetes. A recent study found an even higher number (32.5%), reflecting the changing profile of patients undergoing liver transplant, with the increasingly older patient population.10
The risk of coronary artery disease is particularly high in patients over age 50 and those with coronary risk factors such as diabetes mellitus.7 Other important risk factors include hypertension, existing cardiovascular disease, hyperlipidemia, and smoking. Having 3 or more of these risk factors is associated with higher risks of severe coronary artery disease, major adverse cardiovascular events, and death after transplant.11 Thus, patients who have multiple risk factors should be thoroughly evaluated for severe coronary artery disease, even if they have no coronary symptoms.12
Moreover, older patients currently undergoing liver transplant are also more likely to have concomitant valve disease, which adds further complexity to the management of coronary artery disease in these patients.
Heart failure
Patients with liver disease can develop both cardiac systolic and diastolic dysfunction over time. Other changes in cardiovascular physiology in end-stage liver disease are listed in Figure 1. These patients also have splanchnic and marked peripheral vasodilation with activation of the renin-angiotensin-aldosterone axis. This results in volume overload and elevated pressures in the right ventricle, pulmonary arteries, and left atrium.

Cardiovascular pathology in end-stage liver disease.
LA = left atrial; PA = pulmonary artery; RV = right ventricle; RVSP = right ventricular systolic pressure
Signs and symptoms of heart failure may be masked in patients with cirrhosis, owing to chronic vasodilation, which reduces cardiac afterload, allowing patients to compensate under resting conditions. However, this cirrhotic cardiomyopathy may be unmasked during conditions of cardiovascular stress, such as during liver transplant. Also, after liver transplant, vascular tone promptly returns to normal, with an ensuing increase in venous return, which can further elevate right-sided pressures and precipitate acute heart failure.13 In particular, patients with elevated pulmonary arterial pressure (including those with portopulmonary hypertension), diastolic dysfunction,14 and older age are more likely to develop heart failure after transplant.15
Thus, it is crucial to carefully optimize hemodynamic variables in the perioperative period, particularly preventing volume overload through careful perioperative fluid management and judicious use of diuretics as needed. Of note, however, cirrhotic cardiomyopathy is reversible, and liver transplant can improve left ventricular thickness, diastolic function, and cardiac systolic response to stress over time.16
Other cardiovascular events
Other cardiovascular events such as perioperative arrhythmias and stroke are also common in liver transplant recipients and contribute to higher morbidity and mortality rates after the procedure.17 As a result, liver transplant recipients face a greater risk of cardiovascular events perioperatively, and cardiovascular events are a leading cause of death after liver transplant.18 Thus, reducing cardiovascular risk remains a crucial part of the pretransplant workup in patients with end-stage liver disease.10,17,19 These aspects of perioperative management in liver transplant recipients are discussed further in subsequent sections of this review.
PREOPERATIVE SCREENING FOR HEART DISEASE
History and physical examination
The joint 2012 American College of Cardiology and American Heart Association (ACC/AHA) guidelines for evaluation of cardiac disease in kidney and liver transplant recommend a complete history and physical examination as the first step in evaluating cardiac risk.12 This should focus on any active symptoms of heart disease, risk factors for coronary artery disease, and preexisting coronary or cardiovascular conditions.
Echocardiography for pulmonary hypertension
The 2012 ACC/AHA guidelines note that it is reasonable for patients to undergo echocardiography to look for pulmonary hypertension and intrapulmonary arteriovenous shunting,12 while the 2014 guidelines from the American Association for the Study of Liver Diseases (AASLD) and the American Society of Transplantation (AST) note that it should be done routinely.20 Portopulmonary hypertension (concomitant portal and pulmonary hypertension) is found in 5% to 10% of patients with chronic liver disease.21 Unless patients undergo liver transplant or start on appropriate medical therapy, portopulmonary hypertension carries a very poor prognosis, with 5-year survival rates as low as 14%.21,22
Right heart catheterization
Right heart catheterization should be performed in patients who have evidence of portopulmonary hypertension on echocardiography, to accurately evaluate the severity and etiology of the pulmonary hypertension (defined as mean pulmonary artery pressure ≥ 25 mm Hg, pulmonary capillary wedge pressure ≤ 15 mm Hg, and pulmonary vascular resistance > 3 Wood units on right heart catheterization).12,20 Furthermore, the guidelines recommend consulting a specialist in pulmonary arterial hypertension and considering vasodilator therapy to manage pulmonary hypertension when appropriate if there is no clear secondary cause such as obstructive sleep apnea or left heart disease.
Liver transplant can be offered to patients with portopulmonary hypertension who respond to medical therapy and have a mean pulmonary artery pressure no greater than 35 mm Hg.20
Cardiopulmonary exercise testing
Cardiopulmonary exercise testing and a 6- or 3-minute walk test can provide additional useful prognostic information.20–23 In addition, patients being evaluated for liver transplant should have a cardiac workup to see if they may be at increased risk of myocardial ischemia and infarction perioperatively, so that their risk can be optimized.
Cardiac single-photon emission computed tomography
Cardiac single-photon emission computed tomography (SPECT) has traditionally been a popular choice for the noninvasive ischemic evaluation of patients with a low to moderate risk of cardiovascular events in noncardiac surgery. However, due to the underlying vasodilated state in patients with end-stage liver disease, SPECT can have low sensitivity and specificity as a screening test for coronary artery disease in candidates for liver transplant.12,24,25
Stress echocardiography
The 2013 AASLD/AST guidelines strongly recommend stress echocardiography for cardiac evaluation in liver transplant candidates.20 Recognizing that patients with advanced liver disease are less likely to achieve their target heart rate with exercise, the AASLD/AST guidelines recommend pharmacologic stress echocardiography with a vasodilatory agent such as adenosine, dipyridamole, or dobutamine. Cardiac catheterization in cases in which coronary artery disease cannot be excluded confidently with stress testing.20
Similarly, the 2012 ACC/AHA statement advocates noninvasive testing for coronary artery disease in candidates for liver or kidney transplant being evaluated for coronary artery disease but does not endorse one particular test.12
Dobutamine stress echocardiography remains a commonly used noninvasive tool for preoperative screening for coronary artery disease in liver transplant patients.20 However, it has variable sensitivity in these patients and limited ability to identify those at high risk of cardiovascular events and poor outcomes after transplant.25–27 In view of its limitations, other imaging modalities such as coronary artery calcium scoring and computed tomographic coronary angiography are being investigated for their utility in the cardiovascular evaluation of liver transplant patients, though their exact role is currently less well defined.28–31
Coronary angiography
Coronary angiography is increasingly being used to screen for cardiovascular disease in liver transplant candidates, particularly in those over age 50 and those who have either known coronary disease or risk factors for it.
Other patients who need an invasive assessment for coronary artery disease include those undergoing concomitant cardiac surgery (such as valve surgery) to accurately study the coronary anatomy so that the need for simultaneous coronary artery bypass grafting can be addressed.
Coronary angiography has become safer for patients undergoing evaluation for liver transplant, especially with increasing use of an approach through the radial artery instead of the femoral artery. This approach greatly reduces the risk of vascular complications. Strict emphasis on minimizing dye load and other precautions such as the use of biplane coronary angiography have also reduced the risk of contrast nephropathy.
Team approach
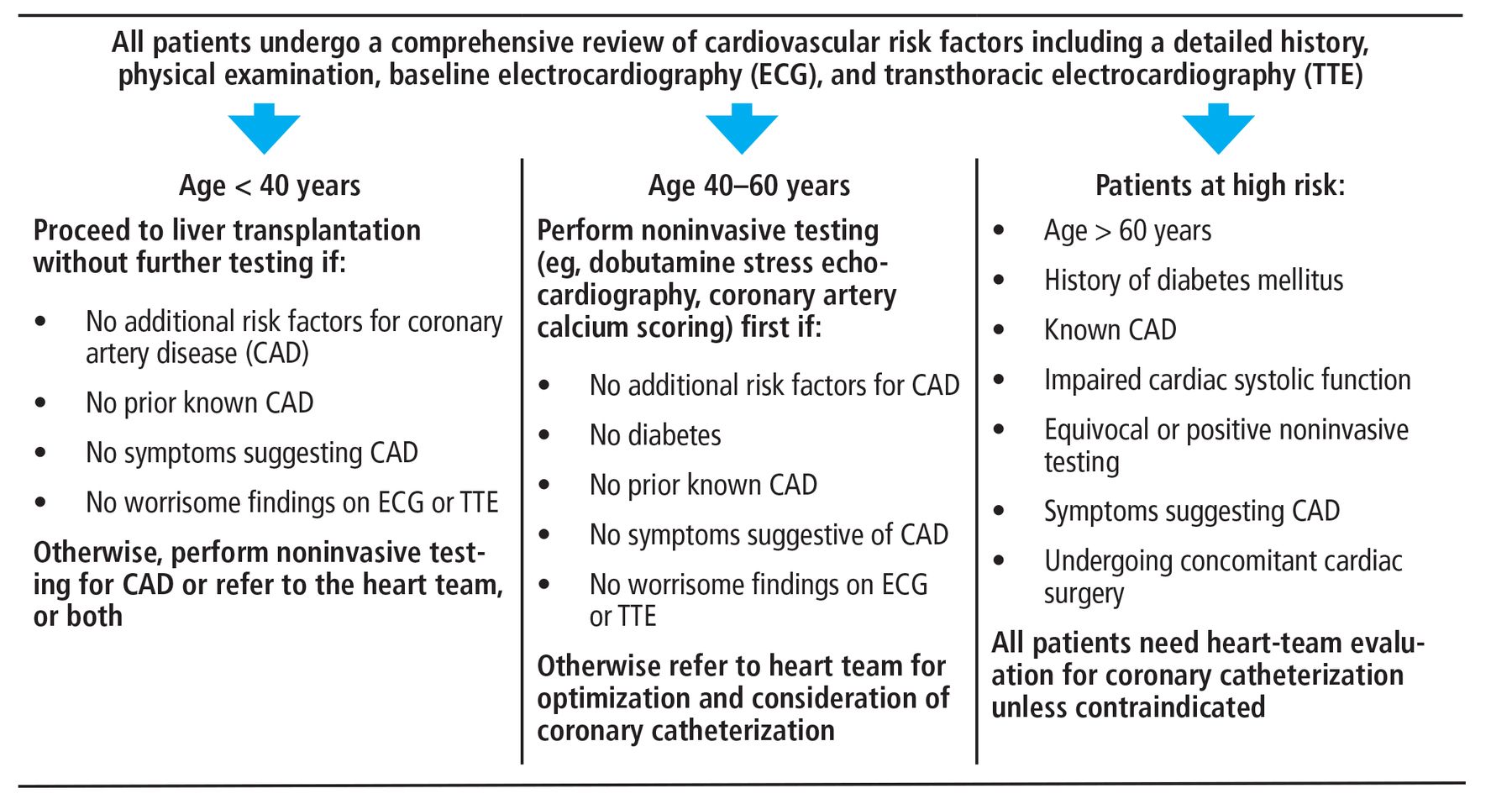
Cardiac evaluation and optimization should ideally be done by a dedicated cardiology team with experience and expertise in managing cardiac issues pertinent to this population,12 particularly to address the need for coronary revascularization and to optimize cirrhotic cardiomyopathy or any coexisting valve disease before liver transplant and to manage cardiovascular events afterward. Figure 2 summarizes the Cleveland Clinic protocol for pretransplant cardiovascular evaluation of patients with advanced liver disease.
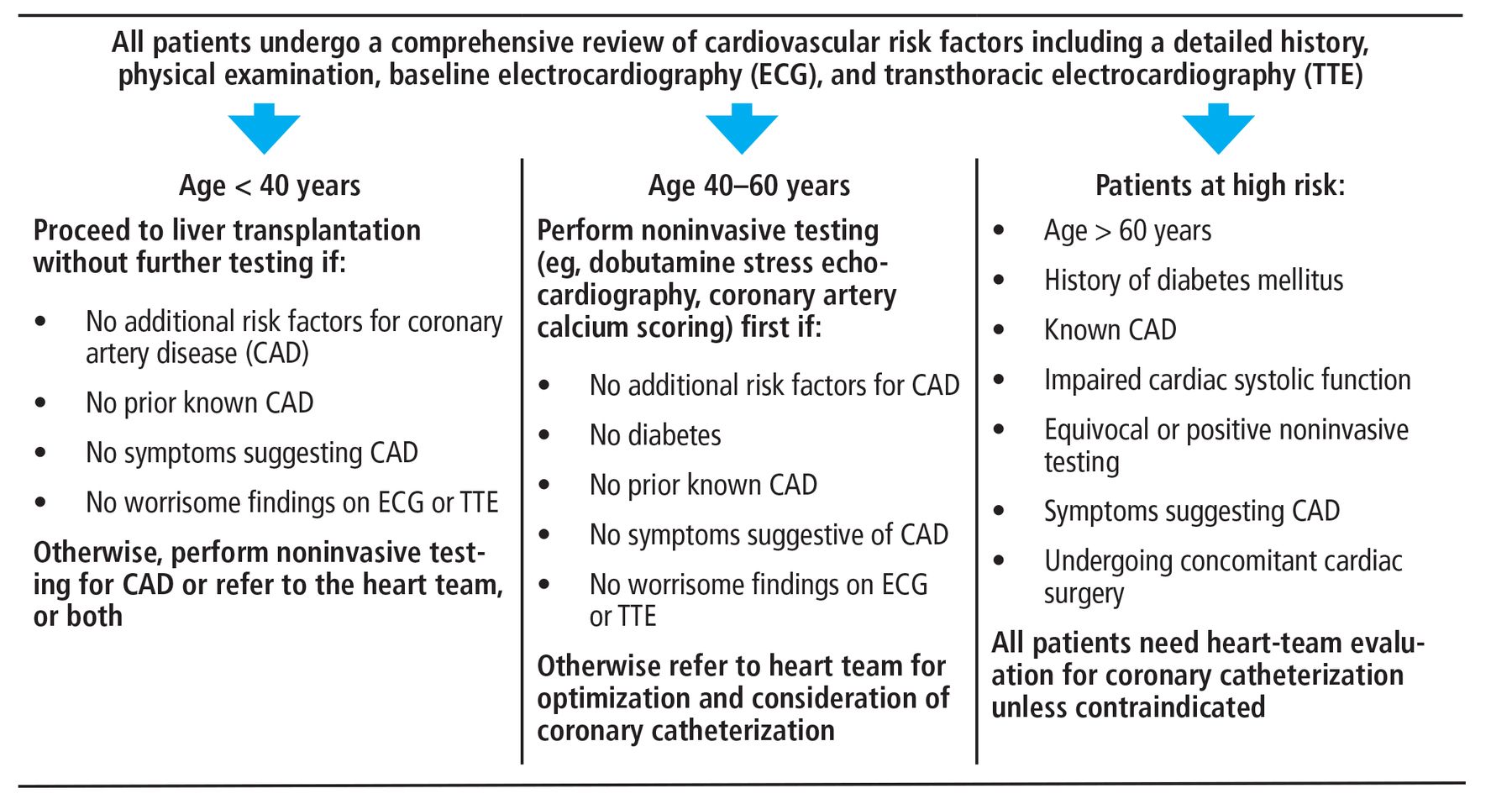
Protocol for cardiac evaluation before liver transplantation at Cleveland Clinic.
CORONARY REVASCULARIZATION BEFORE LIVER TRANSPLANT
Patients with preexisting coronary artery disease have a higher risk of perioperative death and postoperative morbidity after liver transplant, and cardiac events are associated with lower survival rates, particularly in older patients.12 Yet evidence is still currently lacking regarding which patients would benefit from coronary revascularization before liver transplant.
The 2012 ACC/AHA guidelines state that it is reasonable to consider revascularization for patients who have medically refractory angina before liver transplant, while acknowledging the lack of evidence to support this approach.12 Specific indications for revascularization in those without symptoms remain to be established.
Currently, due to the lack of standardized national or international guidelines, the decision about the need for revascularization must be individualized and based on the experience and prevailing practice in each center. More research and clinical trials are critically needed to guide decision-making in this regard.
In patients who undergo percutaneous coronary intervention before liver transplant, the need for dual antiplatelet therapy necessitates delaying the transplant procedure for at least 3 months.12 Further, patients with liver cirrhosis have a higher risk of bleeding complications during dual antiplatelet therapy after percutaneous coronary intervention. However, newer-generation drug-eluting stents may allow for a shorter duration of dual antiplatelet therapy,32,33 thereby allowing earlier transplant and reducing bleeding complications after the coronary intervention.34 Recent studies have shown that with optimal management of coronary artery disease, clinical outcomes can be similar to those in patients without coronary disease.35
VALVE REPAIR BEFORE LIVER TRANSPLANT
Patients with heart valve abnormalities also need careful hemodynamic optimization perioperatively, and those with severe valve disease may need valve surgery (if the operative risk is not otherwise prohibitive) or transcatheter intervention as appropriate. Improvements in transcatheter valve therapy in recent years have expanded the indications for these interventions, and outcomes of transcatheter valve therapy are now comparable to those of surgical valve interventions.
COMBINED HEART SURGERY AND LIVER TRANSPLANT
In some patients, the bleeding risk associated with dual antiplatelet therapy may rule out percutaneous coronary intervention before liver transplant. Furthermore, the coronary anatomy in some patients may be unsuitable for percutaneous intervention, or the coronary disease may be diffuse and therefore impossible to treat with percutaneous intervention.
In addition, some patients may also have coexisting severe valve disease that can only be addressed with cardiac surgery. Such patients have a high risk of perioperative mortality and morbidity if they undergo cardiac surgery or liver transplant alone. For instance, patients with a Child-Pugh score higher than 8 are deemed to have a very high risk of perioperative complications if they undergo cardiac surgery before liver transplant.36
In such patients, concomitant cardiac surgery (or cardiac transplant if appropriate and feasible) and liver transplant can be offered, though the risk of adverse events associated with these procedures is higher in patients with advanced liver disease (Child-Pugh class B and C).12,36 Patients with a high Model for End-stage Liver Disease score or with a short predicted wait-time for transplant cannot wait to undergo at least 3 months of dual antiplatelet therapy after percutaneous coronary intervention. These patients can be offered simultaneous liver transplant and cardiac surgery, provided they do not have specific contraindications, such as left ventricular dysfunction.36
Important contraindications to this combined surgical approach include advanced chronic kidney disease, unfavorable coronary anatomy, active infection, extrahepatic malignancy, evidence of substance abuse, history of nonadherence, and poor social resources.
There are relatively few data in the literature on patients who have undergone simultaneous liver transplant and cardiac surgery.36,37 However, we anticipate that with the increasing age at presentation of patients undergoing liver transplant, such combined procedures may become more common.
Table 1 lists the criteria for combined liver and cardiac surgery at Cleveland Clinic.
Inclusion and exclusion criteria for combined cardiac surgery and liver transplantation at Cleveland Clinic
INTRAOPERATIVE CARDIAC CONSIDERATIONS
Liver transplant is one of the most demanding surgical procedures and is associated with a significant risk of intraoperative cardiovascular complications and therefore poses intraoperative challenges.
Hemodynamic instability
A significant number of patients presenting for liver transplant carry hemodynamic sequelae of end-stage liver disease including generalized vasodilation, low systemic vascular resistance, and an impaired vasoconstrictive response to both endogenous and exogenous vasocon-strictors. Cirrhotic cardiomyopathy has been noted in as many as 60% of patients with cirrhosis.38 These patients also have simultaneous central hypovolemia with splanchnic hypervolemia. The combination of acute blood loss, large fluid shifts, and manipulation of the inferior vena cava during surgery can put a significant stress on the cardiovascular system.
Because of these factors, intraoperative hemodynamic instability is common during the dissection phase (due to blood loss) and the hepatic phase (due to obstruction of the inferior vena cava) of liver transplant.
Postreperfusion syndrome
Immediately after reperfusion of the graft, many patients experience postreperfusion syndrome, defined as a decrease in mean arterial pressure of more than 30% below the baseline value, lasting at least 1 minute, during the first 5 minutes after reperfusion of the graft.39 The reported incidence of postreperfusion syndrome varies widely, ranging from 12% to 77%.40 Up to 5% of patients may experience postreperfusion cardiac arrest.41
Other intraoperative cardiovascular complications
Acute heart failure. Intraoperative heart failure has been reported to occur in up to 3% of liver transplant procedures,42 but that may be an underestimation due to underutilization of intraoperative transesophageal echocardiography.42 Transesophageal echocardiography can be safe and useful for intraoperative monitoring of major life-threatening cardiovascular complications during liver transplant surgery, after carefully reviewing the risks and benefits in each patient.43
Dynamic left ventricular outflow obstruction can develop intraoperatively due to a combination of decreased venous return (due to bleeding, vena cava obstruction, or volume loss due to the drainage of a large amount of ascites) and hyperdynamic left ventricular function. If untreated, it can lead to severe hypotension and hemodynamic instability.44
Takotsubo cardiomyopathy. Stress-induced cardiomyopathy, commonly referred to as takotsubo cardiomyopathy, has been reported perioperatively in the setting of liver transplant and is most commonly seen in female patients. Risk factors for developing stress-induced cardiomyopathy are poorly understood. Management is similar to that for acute heart failure from other causes, with recovery of systolic function expected in a significant percentage of patients.45
Thromboembolism. Right-sided intracardiac thrombosis and pulmonary embolism are other serious thrombotic complications seen during liver transplant and have high mortality rates. Their incidence ranges from 1% to 6%.41,46 Awareness of these common complications during surgery can lead to their prompt recognition, allowing the anesthesiologist to intervene early and prevent a poor outcome.
CARDIAC CONSIDERATIONS AFTER LIVER TRANSPLANT
Acute left ventricular dysfunction can develop after liver transplant, particularly if there is evidence of diastolic dysfunction before transplant.14 Patients who develop acute left ventricular failure after transplant have a high risk of death and graft failure within the first year. Some patients may recover left ventricular function after liver transplant, though recovery is less likely if they have preexisting diastolic dysfunction.14
Heart failure. Patients with evidence of diastolic dysfunction or reduced systolic function before transplant need close postoperative surveillance for signs and symptoms of heart failure. Patients with suspected heart failure or volume overload after transplant should be evaluated with echocardiography, and the cardiology team should be involved early to help manage it.
New coronary artery disease. Liver transplant recipients have an increased risk of developing metabolic syndrome and coronary artery disease after transplant, in particular as a side effect of immunosuppressive regimens.47 For instance, steroids, calcineurin inhibitors, and inhibitors of mammalian target of rapamycin are associated with hyperlipidemia, hypertension, obesity, and diabetes, whereas mycophenolate mofetil and azathioprine appear to have no effect on the risk profile for coronary artery disease.17
Thus, it is important to focus on preventing coronary artery disease after liver transplant in these patients, aggressively modifying risk factors and carefully selecting the immunosuppressive regimen, especially in those who had a moderate to high risk of coronary artery disease before transplant.19 Statins are safe in this patient population. They significantly reduce mortality risk and decrease the risk of graft rejection, yet they remain widely underutilized.48
FUTURE DIRECTIONS
Outcomes after liver transplant, particularly patient and graft survival, have improved with time1 despite a higher risk profile in current patients, who are older and have more cardiac comorbidities than those in the past. Considering the major impact that perioperative cardiovascular events have on outcomes, effective cardiac risk stratification and optimization using standardized and evidence-based protocols could further improve the clinical outcomes of liver transplant.
We anticipate that the use of imaging modalities such as computed tomographic coronary calcium scoring and computed tomographic angiography will expand, in addition to the already rising use of coronary angiography and transcatheter valve interventions in high-risk patients.
Next-generation drug-eluting stents and greater use of transcatheter valve interventions may allow for further improvement in the range of options for cardiovascular optimization before transplant.
Growing knowledge about the risk factors for development and progression of heart failure and coronary artery disease after transplant has also clarified the need for thorough clinical monitoring and effective preventive strategies after liver transplant.
More research is needed into these aspects of cardiovascular care, including screening for heart disease and optimizing cardiovascular health before transplant, managing cardiovascular complications during transplant, and preventing cardiovascular disease afterward.
DISCLOSURES
Dr. Eghtesad has disclosed work as advisor or review panel participant and principal or co-investigator of funded research for Genzyme/Sanofi. Dr. Tong has disclosed consulting, teaching, and speaking for Abbott and Abiomed. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- OLDER PATIENTS, MORE FATTY LIVER DISEASE
- HEART DISEASE IN LIVER TRANSPLANT RECIPIENTS
- PREOPERATIVE SCREENING FOR HEART DISEASE
- CORONARY REVASCULARIZATION BEFORE LIVER TRANSPLANT
- VALVE REPAIR BEFORE LIVER TRANSPLANT
- COMBINED HEART SURGERY AND LIVER TRANSPLANT
- INTRAOPERATIVE CARDIAC CONSIDERATIONS
- CARDIAC CONSIDERATIONS AFTER LIVER TRANSPLANT
- FUTURE DIRECTIONS
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.