


Article Figures & Data
Figures
- Figure 1
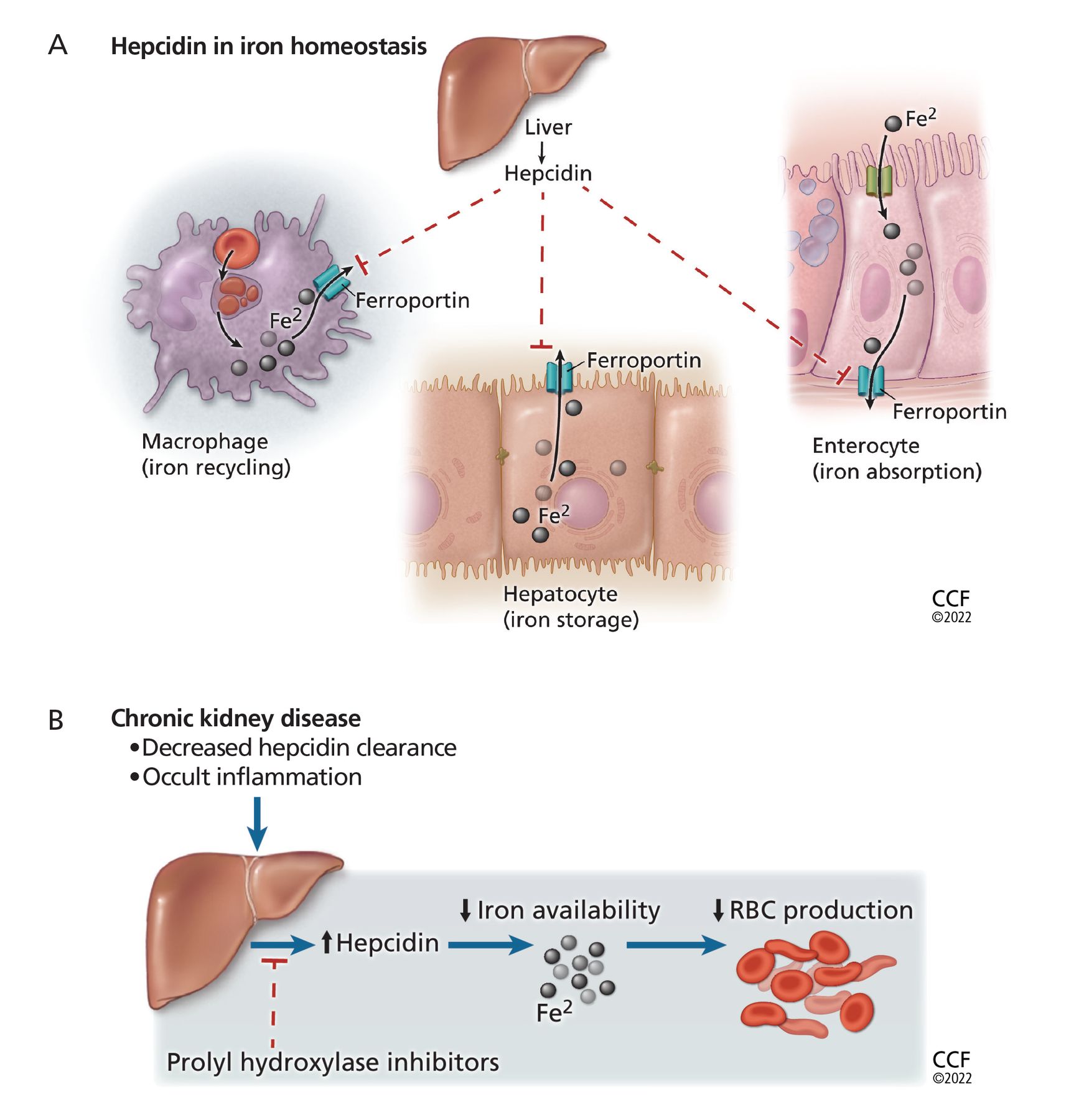
Hepcidin limits erythropoiesis. (A) Hepcidin plays a key role in iron homeostasis. It is produced by the liver and acts to degrade the iron transporter ferroportin, thus preventing release of iron (Fe2) from enterocytes, hepatocytes, and macrophages into the circulation. (B) In chronic kidney disease, hepcidin levels are elevated as a result of the underlying occult inflammatory state and as a result of decreased renal clearance of hepcidin. This makes less iron available for erythropoiesis and can lead to resistance to erythropoiesis-stimulating agents. Prolyl hydroxylase inhibitors (PHIs) decrease liver production of hepcidin, which may improve iron metabolism and lead to efficient management of anemia of chronic kidney disease. (RBC = red blood cell.)
- Figure 2
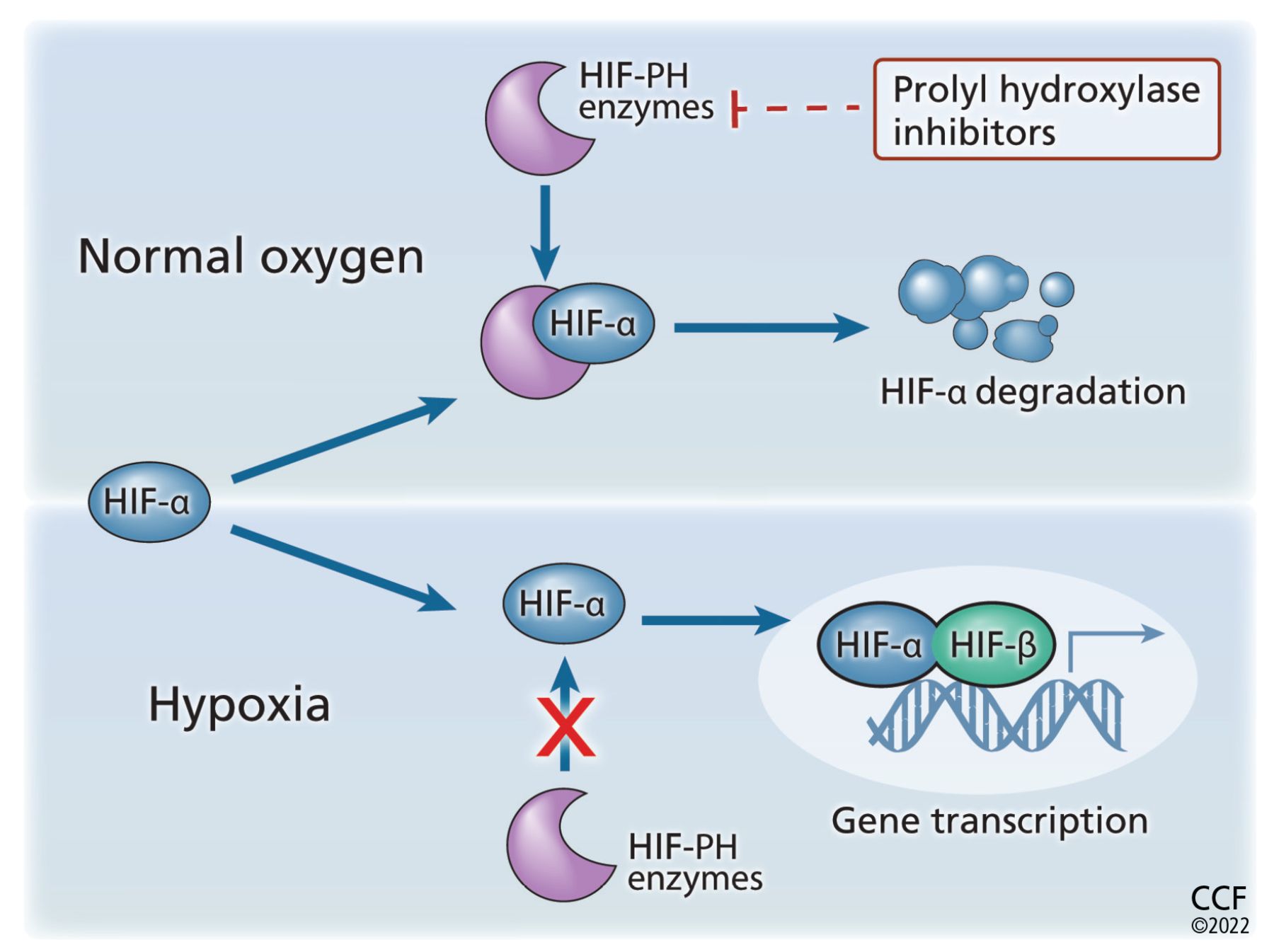
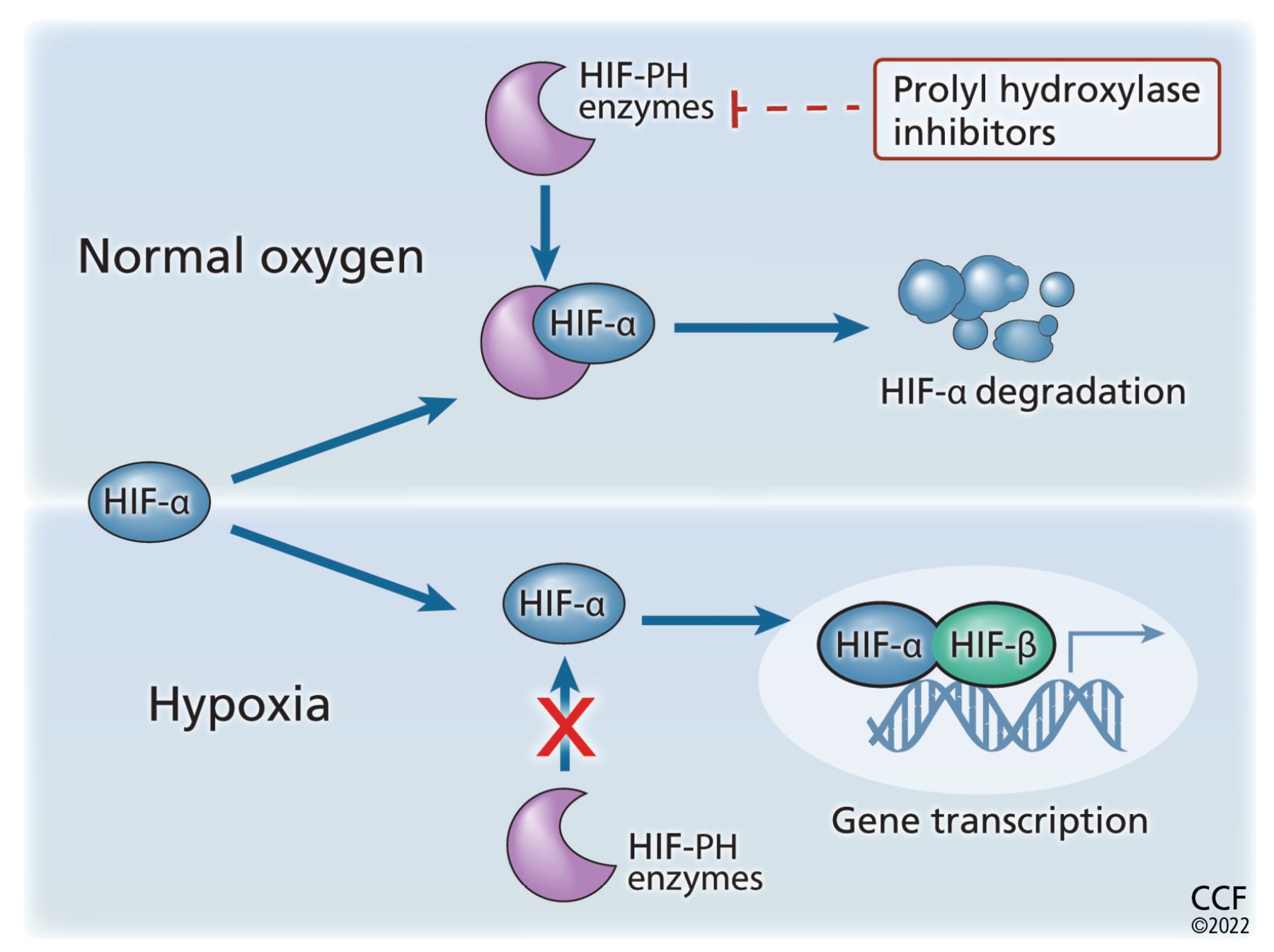
Prolyl hydroxylase (PH) inhibitors increase erythropoiesis. Hypoxia-inducible factor (HIF) is a heterodimer consisting of 2 subunits, alpha and beta (HIF-α, HIF-β). Undernormal oxygen tension, the proline residue of HIF-α is hydroxylated and subsequentlydegraded. This prevents the formation of the heterodimer and stops subsequent erythropoietin transcription. When oxygen tension is low, HIF-α is not degraded, thus allowing HIF heterodimers to form. This leads to an increase in erythropoietin transcription. By preventing hydroxylation of HIF-α, PHIs prevent its degradation and stabilize the HIF-α/HIF-β heterodimer. This leads to increased downstream gene expression with increased production of endogenous erythropoietin.
Tables
- TABLE 1
Clinical trials of erythropoiesis-stimulating agents to increase hemoglobin to different targets in chronic kidney disease
Trial Normal HCT21 CHOIR22 CREATE23 TREAT24 Population Patients with chronic heart failure and end stage kidney disease on dialysis (N = 1,233) Chronic kidney disease (N = 1,432) Chronic kidney disease (N = 603) Chronic kidney disease with diabetes (N = 4,038) Hemoglobin targets 10 vs 14 g/dL 13.5 vs 11.3 g/dL > 13 vs 11 g/dL > 13 vs 9 g/dL Target achieved? No No Yes No Primary outcomes Time to death or first myocardial infarction Composite of death, myocardial infarction, hospitalization for chronic heart failure, stroke Time to first cardiovascular event Composite of death or a cardiovascular event, or
Composite of death or end-stage kidney diseaseResults with higher outcome hemoglobin target Higher risk of primary outcomea Higher risk of primary outcomeb Trend toward higher risk of primary outcome (not statistically significant) No increase or reduction in risk of primary outcome Other results with higher target Higher rate of thrombosis Improved quality of life Higher rates of stroke and malignancy- associated mortality; less need for blood transfusions ↵a Risk ratio 1.28, 95% confidence interval 1.06–1.56, P = .01.
↵b Hazard ratio 1.34, 95% confidence interval 1.03–1.74, P = .03.
CHOIR = Correction of Hemoglobin and Outcomes in Renal Insufficiency trial; CREATE = Cardiovascular Risk Reduction by Early Anemia Treatment With Epoetin Beta trial; HCT = hematocrit; TREAT = Trial to Reduce Cardiovascular Events With Aranesp Therapy
Adapted from Nakhoul G, Simon JF. Anemia of chronic kidney disease: treat it, but not too aggressively [published correction appears in Cleve Clin J Med 2016; 83(10):739]. Cleve Clin J Med 2016; 83(8):613–624. doi:10.3949/ccjm.83a.15065 with permission from the Cleveland Clinic Foundation © 2016.
Benefits Higher hemoglobin levels18 Decreased blood transfusion needs29 Better quality of life23,30–32 Reduction in left ventricular hypertrophy33 Risks Cardiovascular events21,24 Malignancy-associated mortality24 Thromboembolic events21,24 Hypertension21–24 Hemodialysis vascular-access thrombosis21 Drug Half-life (hours) Dosage in adults Intravenous Subcutaneous First-generation Epoetin alfa36 4–13 5–24 Initial 50–100 U/kg 3 times weekly intravenously or subcutaneously
Maintenance individualizedSecond-generation Darbepoetin alfa37 21 35–139 Initial 0.45 μg/kg weekly, adjusted as needed to maintain hemoglobin 11–13 g/dL
Do not adjust dose more frequently than once a month unless clinically indicatedThird-generation Methoxypolyethylene glycol–epoetin beta38 119 124 Initial 0.6 μg/kg every 2 weeks intravenously or subcutaneously Epoetin zeta39 Similar to first-generation epoetin alfa Trial No. Patients Effect on hemoglobin Besarab et a44 104 Not on dialysis Better than placebo Chen et al45 154 Not on dialysis or ESAs Better than placebo ANDES46 922 Not on dialysis or ESAs Better than placebo OLYMPUS47 2,781 Not on dialysis Better than placebo ALPS48 594 Not on dialysis or ESAs Better than placebo Besarab et al51 60 On dialysis, or ESAs Better than baseline Chen et al52 305 On dialysis and ESAs As good as epoetin alfa HIMALAYAS54 1,043 New to dialysis As good as epoetin alfa Akizawa et al66 303 On dialysis As good as darbepoetin alfa Akizawa et al67 56 On dialysis Better than baseline Akizawa et al68 239 On dialysis Better than baseline in those not on ESAs Akizawa et al69 99 Not on dialysis or ESAs Better than baseline Provenzano et al70 145 Not on dialysis Better than baseline Provenzano et al71 90 On dialysis As good as epoetin alfa ESA = erythropoiesis-stimulating agent
Expanded Table 4
Published phase 2 and 3 trials of roxadustat
Files in this Data Supplement:
- Expanded Table 4 - Published phase 2 and 3 trials of roxadustat
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- HOW CHRONIC KIDNEY DISEASE LEADS TO ANEMIA
- ESAs ARE THE MAINSTAY, BUT HAVE LIMITED BENEFIT
- A NEW CLASS OF DRUGS: PROLYL HYDROXYLASE INHIBITORS
- TRIALS OF THE NEW AGENTS IN PATIENTS NOT ON DIALYSIS
- TRIALS IN PATIENTS ON DIALYSIS
- BENEFITS AND SIDE EFFECTS OF PHIs
- PHI DRUGS: CURRENT STATUS
- KEY QUESTIONS REMAIN
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics